
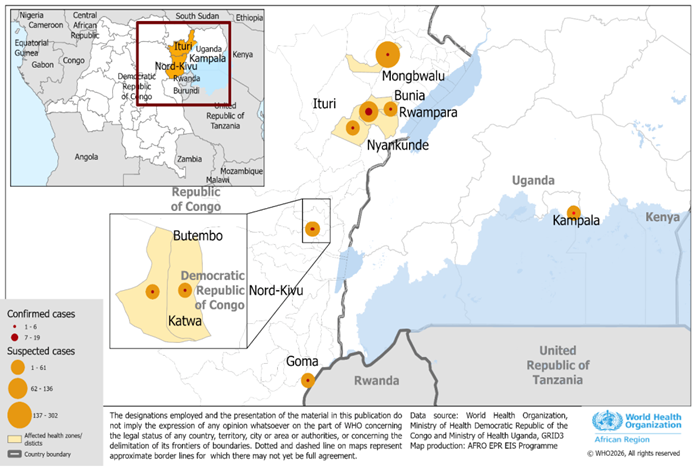
On 15 May 2026, the Democratic Republic of the Congo (DRC) declared an outbreak of Ebola disease caused by Bundibugyo virus (BDBV) in Ituri province. This is the country’s 17th Ebola outbreak but already one of the most severe with inter-provincial and cross-border spread. On 15 May, Uganda confirmed an imported case involving a patient who had travelled from Bunia for care and additional cases have since been identified. On 17 May, authorities in Goma, North Kivu, also confirmed a case connected to the Ituri outbreak. The Director General of WHO declared the outbreak a Public Health Emergency of International Concern on 17 May.
This summary note details relevant contextual factors in Ituri Province, with a focus on three of the currently most affected health zones: Mongwalu, Bunia and Rwampara. Health zones are the main administrative units of the DRC health system; there are 519 nationally and 36 in Ituri province. Mongwalu is a semi-rural area with artisanal mining sites, Bunia is the provincial capital, and Rwampara is a health zone on the outskirts of Bunia.
Population, language and ethnicity
- Population: Ituri has a population of 7 million, of which 13% are internally displaced. Ituri is geographically diverse, with a high plateau, large tropical rainforest (Ituri Rainforest), and savannah. It has a provincial capital city (Bunia) and towns, connected to gold mining and commercial activities, with informal settlements. The province is also home to internally displaced camps, and gold mining settlements (e.g., Mongbwalu). The rainforest region is home to the vulnerable Mbuti – an indigenous group that relies on hunting and gathering.
- Urban centres and urban connections: The provincial capital Bunia (including the wider urban area) is home to nearly 1.5 million inhabitants and has a long history as a ‘humanitarian hub’ dating back to the second Congo war (1998-2003). As a commercial hub, Bunia is important for rural-urban and regional trade, especially to Uganda. It is a transport and logistics hub for agricultural and mining exports, as well as consumer imports from Uganda. It connects rural territories within Ituri to urban markets. Bunia is connected to other commercial hubs including the larger city of Butembo in North Kivu, and Beni – an important urban centre located between the two cities. Strong social and economic ties, particularly familial ties, link the cities’ populations. Bunia is more ethnically and linguistically mixed than other more rural areas of Ituri, including large numbers of IDPs who have come to Bunia displaced by violence.
- Ethnic identities: Ituri is highly heterogeneous, with at least 18 ethnic groups. The largest include Hema, Lendu, Alur and Lugbara, alongside smaller groups such as Bira, Nyali, Lese and Ndo-Okebo. Ethnic identity has become increasingly politicised, with the additional category of “non-originaires” (e.g. Nande traders from North Kivu) reflecting tensions around belonging, economic competition, and political influence.
- اللغات: Swahili is the most common language in Ituri. Lingala is widely used as the language of the army, administration, radio and television. French is the language of elites, higher education, and administration. It is only partially understood by populations with a limited education. There is great linguistic diversity, particularly in the villages e.g. the Hema languages (around Rwanpara), Nyali, Lendu (around Mongwalu). Swahili is the lingua franca within the mining operations.
- Communication: In some parts of Ituri, it can take 2-3 days to relay information due to a lack of network coverage. Mobile and internet coverage is better in Bunia and major towns, whereas rural areas (e.g., Djugu, Irumu) rely on basic mobiles and solar-powered community networks or satellite-based networks. Social media use is higher in urban centres.
Security, conflict and politics
- Military government: Since May 2021, a military administration has been in place in Ituri to fight insecurity.
- Ituri conflict and Lendu-Hema tension: The long running violent conflict between the Lendu and Hema that dates from the 1999-2003 war continues in Ituri, and recent clashes have led to further deaths and displacement. Contested claims to indigeneity shape struggles over land and authority. These tensions are rooted not only in livelihoods (often simplistically framed as pastoralist vs farmer) but in historical processes of governance and exclusion.
- Multiple armed factions: Armed factions continue to use ethnic affiliations to recruit combatants and to acquire economic and political power. Each ethnic group has its own armed group. There are groups for the Hema (Zaire), the Lendus (north: CODECO with its factions; south Lendu: the FRPI), the Nyali-Kilo (Chabakulawatu), the Bira (FPIC/Chini ya Kilima), and the Lese (Chini ya Tuna). ADF (Allied Democratic Forces) is an armed group of Ugandan origin, founded in 1995, operating from eastern DRC, affiliated with the Islamic State in Central Africa, perpetuating violent attacks against civilians. NSAGs are implicated in regional dynamics with alleged support from national actors. M23 is not active in Ituri but M23 controls Goma and the southern part of North Kivu. Cases have been confirmed in North and South Kivu. Certain administrative entities in Ituri province are outside state control. Health cooperation between belligerents will be an important question raised by this epidemic.
- Bunia / Mongwalu axis: The security situation is precarious and marked by chronic insecurity and many abuses against local populations; though it is less tense than in North Kivu in 2018 (a period of presidential transition and regime change), the area is still highly insecure and has deteriorated over the last two years, in part as a consequence of changes in M23 control and Government of DRC responses in the Kivus. However, the constitutional revision currently under discussion in the DRC could become a point of tension to monitor.
- MONUSCO: The UN peacekeeping mission remains active in Ituri.
- Historical legacies: Colonial ‘divide and rule’ approaches have entrenched ethnic hierarchies that continue to shape patterns of inequality and grievance. This will influence how external interventions are perceived.
- Fluid and instrumentalised identities: Ethnic affiliations are often mobilised strategically by local elites, armed actors and political movements. Groups may shift alliances pragmatically, leveraging external actors (including state and international interventions) to consolidate power.
- Competition and response risks: Economic tensions (including with ‘non-originaires’) intersect with fragmented authority and patronage networks, meaning response activities (e.g. jobs, contracts, services) may be politicised or perceived as biased, affecting trust and engagement.
الرعاية الصحية
- Health facilities under strain: According to the Health Cluster, 17 partners support 107 health facilities across Ituri. Infection Prevention Control (IPC) readiness remains critically low with assessments showing only 34% coverage at Mongbwalu General Referral Hospital, and less than 7% in other facilities. There are severe shortages of personal protective equipment (PPE), IPC materials, triage capacity and isolation space.
- Systematic looting and destruction of health centres: Targeting of healthcare is widespread in eastern DRC. There were over 100 attacks against health workers in Ituri in 2025. There were widespread attacks against health workers and facilities in the Ebola outbreak in the region in 2018-20.
- Financial barriers: There are many healthcare options, especially in Bunia, including biomedical and faith-based practices. However, quality care is costly and a person’s financial means often determines where and when they seek care. The wealthiest seek treatment abroad (Uganda, Kenya).
سبل العيش
- Informal sector: Most people work in the informal sector, including informal mining, and subsistence farming. Cross-border and local market trade is a key source of income for border communities.
- Gold mining: Artisanal gold mining supports the economy of the whole province. It requires a large labour force that are mobile and work under very precarious conditions. It is also seasonal – during the rainy season, some will change jobs and livelihoods. Mining is organised around networks of “big men” (people with capital to invest and connexions to networks of intermediaries locally and in political centres) who are important entry points for the response. Interrelated dynamics of coercion and loyalties through economic mining networks constitute key power structures to map out.
Internal mobility
- The population is highly mobile: There is constant movement between the extraction sites where miners work and Bunia, the town where families are settled. Bunia is also the city that people flee to for shelter from the insecurity before returning to their villages, though it is also insecure.
- الإزاحة as a result of conflict is the biggest driver of internal displacement in Ituri.
- Fuel: Unlike in other rural areas of DRC, access to money due to the gold mining means that some people have the means to buy fuel. However, fuel crisis as a result of the Strait of Hormuz could reduce both supply and purchasing power.
- Revenue for armed factions: A major source of revenue for the state and armed factions in the region comes from taxing goods and people moving along the province’s main roads.
- Repatriation: After death, a person will be repatriated to their home villages for burial.
International mobility
- International borders: Ituri province borders Uganda and South Sudan.
- تجارة: Trade in Ituri is deeply connected with Uganda. The Goli–Mahagi–Bunia Road is central as it connects Ituri with Uganda and also with Kenya, through the Northern corridor. Informal cross-border trade is prevalent.
- Commodities: The main exports are gold, coffee, timber and cacao. The main imports are manufactured goods.
- Border closure: The border between Goma and Rwanda was closed after the confirmation of a case in the city.
Vulnerable populations
- Humanitarian need: Before the outbreak, 1.9 million people were already in need of humanitarian assistance in Ituri, including more than 900,000 internally displaced people who have additional vulnerabilities that may heighten risk of infection, including very limited access to water and sanitation.
- Women: Early reports suggest that women account for two thirds of suspected cases, which is consistent with data from previous outbreaks: they are at risk of being infected through direct contact whilst caring for the sick. There are very high levels of GBV in Ituri as well as CRSV.
- Health workers: At least four healthcare worker deaths have been recorded as suspected Ebola deaths since the start of the current outbreak, highlighting the risk of healthcare-associated transmission and the importance of PPE and adherence to protective measures for care providers.
- Transactional sex: Transactional sex as a livelihood strategy is common in mining areas and women may face elevated risks if sexual transmission of Bundibugyo virus is possible (as with Zaire ebolavirus). Risks would include both commercial and less visible forms of transactional sex, both of which are shaped by women’s economic marginalisation.
موارد – please refer to collected SSHAP resources. For further reference, a detailed Open Access contextual note on Ituri has been developed by regional experts, convened by Jules Villa from Institut Pasteur and is available online in French و in English.
مؤلفون – Jules Villa (Institut Pasteur), Annie Wilkinson (IDS) and Juliet Bedford (Anthrologica). Further revisions by Megan Schmidt-Sane (IDS) and Diane Duclos (LSHTM).
Funding Acknowledgement – This brief has been produced for the Multi-Hazard Research Network (MHRN), funded by the UK Foreign Commonwealth and Development Office.


 لمواصلة دراستهم الثانوية تعليم. يعد فحص درجة الحرارة جزءًا من بروتوكولات السلامة الصارمة التي يتم تنفيذها في جميع المدارس في جميع أنحاء البلاد، لتقليل خطر انتقال مرض فيروس الإيبولا (EVD) في المدرسة. وافتتحت أكثر من 1000 مدرسة إعدادية اعتبارًا من 30 مارس لأكثر من 275200 طالب الجلوس لامتحانات شهادة التعليم الأساسي. في مارس/أبريل 2015 في سيراليون، بينما تستعد المدارس في جميع أنحاء البلاد لإعادة فتح أبوابها بعد ثمانية أشهر من الإغلاق بسبب أزمة مرض فيروس الإيبولا، تعمل الحكومة واليونيسف والشركاء على ضمان بقاء الأطفال آمنين من خلال الحد قدر الإمكان من مخاطر انتقال مرض فيروس الإيبولا. ومن المقرر إعادة فتح المدارس - التي ظلت مغلقة في جميع أنحاء البلاد بعد العطلة بين يوليو وأغسطس - في 14 أبريل، حيث من المتوقع أن يستأنف حوالي 1.8 مليون طالب دراستهم. ولدعم عودة الطلاب، قامت اليونيسف بتيسير تدريب 9000 معلم على تنفيذ بروتوكولات السلامة لتقليل مخاطر انتقال العدوى في المدارس، بما في ذلك قياس درجات حرارة الأطفال عند وصولهم إلى المدرسة وجعلهم يغسلون أيديهم قبل دخول الفصل الدراسي. وتدعم اليونيسف أيضًا توزيع مواد النظافة ومعدات التنظيف لإعداد المباني المدرسية وتقليل فرص الإصابة بالعدوى؛ وتوفر 24,300 محطة لغسل الأيدي (حوالي ثلاث لكل مدرسة)، بالإضافة إلى 1.8 مليون مجموعة مدرسية ودعم نفسي واجتماعي للطلاب. وتدعم اليونيسف أيضًا أنشطة التعبئة الاجتماعية لرفع مستوى الوعي، وبرامج التعليم الإذاعي الحكومية اليومية في حالات الطوارئ للسماح للأطفال بمواصلة التعلم في المنزل خلال أزمة الإيبولا، ووزعت حوالي 17000 جهاز راديو يعمل بالطاقة الشمسية على الأطفال في المناطق الريفية.")