
This systematic review examined peer-reviewed and grey literature to document global best practices for effective public health emergency response by EOC.
A systematic review of public health emergency operations centres (EOC)

This systematic review examined peer-reviewed and grey literature to document global best practices for effective public health emergency response by EOC.

Although in parts of South Sudan the situation is unstable which necessitates humanitarian action, in other parts of the country development programmes are taken up with the communities.
In Northern and Western Bahr el Ghazal states, Aweil North and Wau county respectively, the South Sudan Health Action and Research Project (SHARP) works on improving reproductive health.

The spread of Ebola in West Africa centres on a region with a shared recent history of transnational civil war and internationally led post-conflict reconstruction efforts. This legacy of conflict and shortcomings in the reconstruction efforts are key to understanding how the virus has spread. The dynamics of warfare tied into and accentuated the state’s remoteness from many people. Ebola has simply unmasked persisting deep public suspicion and mistrust of the state, laying bare the limits of post-conflict reconstruction to transform state-society relations.
The reconstruction emphasis on rehabilitating pre-existing governance structures – such as the paramount chieftancy in Sierra Leone – did not redress deeply rooted social inequalities, with the result that many people have been marginalised. Ebola’s impacts threaten to undo some of the advances made since the wars ended in Sierra Leone and Liberia, yet there are critical lessons to learn about how to better support societies shaped by violence and war.

This issue of Frontiers of CLTS explores the potential, and some of the recorded learning, on how CLTS, as a community-based, collaborative approach to sanitation behavioural change, can be applied successfully in contexts of fragility and displacement, leading to communities more convinced and prepared to maintain and develop safe sanitation practices.

This issue of Frontiers of CLTS brings together lessons on violence related to sanitation and hygiene and examples of good practice from a range of contexts including urban and humanitarian as well as rural.
It interprets these lessons to propose good practice for CLTS practitioners in how they can contribute to reducing vulnerabilities to violence through the ways they work.

The origin of the Ebola outbreak in West Africa has been traced to the likely confluence of a virus, a bat, a two-year-old child and an under equipped rural health centre. Understanding how these factors may have combined in south-eastern Guinea near the end of 2013 requires us to rethink elements of the familiar Ebola ‘outbreak narrative’, as propagated by the international media, in a deeper political, economic and ecological context. This includes examining the social, ecological and epidemiological evidence and questioning long-held and misplaced assumptions about rural resource users, rural livelihoods, deforestation and environmental change, and the role of development in both the current crisis and in realising a more resilient future.
Emerging research indicates that demography, patterns of land use and of human-wildlife interaction are all implicated in zoonotic ‘spillover’ events, but cannot be generalised across cases and localities.

Containment strategies for Ebola rupture fundamental features of social, political and religious life. Control efforts that involve local people and appreciate their perspectives, social structures and institutions are therefore vital. Unfortunately such approaches have not been widespread in West Africa where response strategies have been predominantly top-down. Authoritarian tactics have had questionable effect, potentially worsening the epidemic and contributing to social and economic burdens. Failure to involve local people and their concerns is often justified by budgetary and practical restraints such as lack of time and resources.
However, some of the current Ebola responses reflect problematic assumptions about local ignorance and capability. These sentiments are deeply rooted, having evolved with unequal power dynamics over long periods of time. The emerging evidence on successful local responses suggests that local populations can learn rapidly to adjust high-risk traditional practices and reduce transmission in conjunction with solid public health measures.
The economic effects of the Ebola health crisis are slowly unfolding as the virus continues to affect Sierra Leone, Liberia and Guinea. The most important sector is mining as these three countries share a rich iron ore geological beltway. The macroeconomic impacts of the crisis came into sharp focus when London Mining, Sierra Leone’s second largest iron ore producer, suspended its activities.
Ebola is also having a devastating impact on the informal mining sector, which provides a livelihood to some of the country’s poorest people. However, how the effects of mining have left countries vulnerable to the Ebola crisis also deserves attention. Large-scale mining creates social and ecological disruptions that could encourage the emergence and spread of disease. External mining interventions have also fuelled suspicion by local populations of foreign and government interventions, as they have received so few benefits from the mining resource boom.

Over the last decade, the avian influenza virus, H5N1, has spread across most of Asia and Europe and parts of Africa. In some countries – including Indonesia, China, Vietnam, Bangladesh, Nigeria and Egypt – the avian disease has probably become endemic. There has, as yet, been no human pandemic, although 245 deaths have been reported since 2003. A major international response has been launched, backed by over $2 billion of public money. Huge numbers of poultry have been culled, vaccination campaigns have been implemented and markets have been restructured. These efforts have affected the livelihoods and businesses of millions. In addition, substantial efforts have been invested in improving human and animal health systems, combined with major investments in drug and vaccine development.
Detailed contingency and preparedness plans have been devised in case a pandemic occurs. This paper asks: what lessons can we learn from this experience,

Current global health policy is dominated by a preoccupation with infectious diseases and in particular with emerging or re-emerging infectious diseases that threaten to ‘break out’ of established patterns of prevalence or virulence into new areas and new victims. This paper seeks to link a set of dominant narratives about epidemics and infectious disease with what is often called the architecture, or organizational landscape, of global health policy. A series of dichotomies helps to distinguish and valorise epidemics policies. Fast- versus slow-twitch models of disease, global versus local models of culture, and official versus unofficial models of knowledge provide categories according to which policies can be evaluated, designed and implemented. As a result, policy on the global scale has tended to be oriented towards addressing highly time-focussed outbreaks that threaten to cross international boundaries rather than longer-term endemic problems the affect the most vulnerable people.

Based on a household survey in Indian Sundarbans hit by tropical cyclone Aila in May 2009, this study tests for evidence and argues that health and climatic shocks are essentially linked forming a continuum and with exposure to a marginal one, coping mechanisms and welfare outcomes triggered in the response is significantly affected. The data for this study is based on a cross-sectional household survey carried out during June 2010. The survey was aimed to assess the impact of cyclone Aila on households and consequent coping mechanisms in three of the worst-affected blocks (a sub-district administrative unit), viz. Hingalganj, Gosaba and Patharpratima. The survey covered 809 individuals from 179 households, cross cutting age and gender. A separate module on health-seeking behaviour serves as the information source of health shocks defined as illness episodes (ambulatory or hospitalized) experienced by household members.
Finding reveals that over half of the households (54%) consider that Aila has dealt a high,

Throughout sub-Saharan Africa, the human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS) pandemic is having devastating and tragic social, economic, and political impacts. HIV/AIDS is both a health issue and a development problem, with complex links to rural livelihoods, human capacity, and natural resource conservation. As the HIV/AIDS pandemic in Sub-Saharan Africa has spread, it appears that increased pressure has been placed on the already dwindling forest resources on which vulnerable populations depend. Evidently, forests and the products that they provide may well decrease the vulnerability of rural people by increasing their resilience to HIV/AIDS. Yet, despite decades of research regarding the impacts of HIV/AIDS on rural livelihoods in Sub-Saharan Africa, the links between HIV/AIDS, vulnerability, resilience, and wild natural capital has largely gone unexplored. Research on the interactions between the use of forest resources and contemporary epidemics in general, and on the environmental dimensions of the HIV/AIDS pandemic in particular,

More than 70 million people died in famines during the 20th century. This paper compiles excess mortality estimates from over 30 major famines and assess the success of some parts of the world – China, the Soviet Union, and more recently India and Bangladesh – in apparently eradicating mass mortality food crises. This is contrastes with the experience of sub-Saharan Africa where famines precipitated by adverse synergies between natural triggers (drought) and political crisis (civil wars) have become endemic since the late 1960s.
The paper also examines the evolving discourse around famine causation during the century, and finds that despite the proliferation of demographic, economic and political theories, each embodies the reductionist perspective of disciplinary specialisation. The paper concludes by arguing that if famine is to be completely eradicated during the 21st century this requires not just technical (food production and distribution) capacity but substantially more political will,

The paper discusses strategies for meeting the needs of the poor in a pluralist health sector. It argues that the first step in defining such strategies must be a realistic assessment of the complex and unregulated market for health services that exists in many parts of Africa. It suggests that simplistic calls for government and donors either to cease or substantially increase funding for existing public health services are misguided in a situation where even the labels ‘public’ and ‘private’ require careful analysis. Instead it proposes that governments should use their resources and influence to promote the substantial changes required to establish effective health services.
It also calls for a fundamental reassessment of the relationship between government, health services providers, civil society organisations, communities and households in the health sector. It concludes that a new vision for pro-poor health services will emerge from a process of listening to the needs of the poor,

This thesis examines the Influenza A/H5N1 virus in action through an ethnographic study focused on the entwined concepts of risk and modernity. The objective is to explain why the response to the virus has been challenged in Indonesia.
Concerned with policy formulation, and everyday practice, the thesis argues that assemblages of historical, political, institutional and knowledge‐power processes create multiple hybrid constructions of risk and modernity, which challenge technical responses based on epistemological positions and institutional arrangements that do not allow for such hybridity.

As a country suffering from large-scale AI outbreaks and receiving considerable international support, Vietnam provides a crucial case not to be missed in any analysis of the global AI crisis. Vietnam is also interesting because of two paradoxes in her response to AI. Despite being poor, Vietnam selected the most expensive approach (comprehensive vaccination) to disease control. Despite substantial foreign aid and praise lavished on Vietnam, and despite a tough strategy, Vietnam has not performed better than neighbouring countries in keeping the epidemic from coming back. Based on interviews of various stakeholders and newspaper sources since 2003, this paper analyses the timeline of major events, key narratives driving the debate, and the main actor networks in the policy process.
The author found Vietnam’s AI policy process was characterised by top down/technical perspectives supported by the central government and foreign donors. These narratives reinforced the political interests of a national/international elite.

This working paper reviews some of the main methodological approaches to emerge in the 1990s, reflecting on both their objectives and their limitations.

The problem of HIV internationally has many wide ranging impacts on people, communities and countries’ development. In the last decade antiretroviral (ARV) treatment has emerged as the major scientific-technical solution, albeit a costly one. Access to ARV treatment is of vital importance across Africa and around the world. Resources for HIV treatment, care and support are transferred globally on a massive scale. However, how such programmes operate ‘on the ground’ in different contexts is still unclear. This research contributes to understanding the experience of the people who access such treatment programmes in different contexts. This research focuses on this gap, exploring how treatment programmes are experienced, how the availability of treatment impacts both on people’s experience of being HIV+ and how the availability of treatment may also change perceptions of what it means to be HIV+, both individually and at a societal level.

Examining the political economy of knowledge in responses to the 2009-10 influenza pandemic, this paper argues that globally, and in many individual nations, techno-scientific narratives constructed by bio-medical actor networks failed to correspond with the more variegated narratives of multifarious global publics, and so struggled to recruit support and maintain credibility and authority.With reductive narratives constructed by bio-medical actor networks confounded by the uncertainties intrinsic to the influenza virus, the complexities of the disease in individuals, and compromised by continuing ignorance, political and cultural forces became dominant.Universalistic, one-size-fits-all responses drawn from reductive science are therefore argued to be insufficient, and possibly misguided. Planning and response efforts must consider diverse local settings and concerns. Reductive technical framings emerging from tight, unreflexive actor networks may prevent other options from emerging, and limit response pathways.
Such narrow,technocratic responses are not only at odds with the varied understandings,

The international response to Ebola has been decried for being ‘too slow, too little, too late’. As well as racing to respond, we need to consider what has happened over the past decades to leave exposed fault lines that enabled Ebola to move so rapidly across boundaries of people’s bodies, villages, towns and countries. Gender is important to these fault lines in two related spheres. Women and men are differentially affected by Ebola, with women in the region taking on particular roles and responsibilities as they care for the ill and bury the dead, and as they navigate ever-diminishing livelihood options and increasingly limited health resources available to pregnant women.
Furthermore, structural preconditions in ‘development’ itself have deepened these gendered fault lines. A currently powerful set of ideas in gender and development discourse locates certain patterns of ‘non-modern’ gender relationships as the root cause of poverty and underdevelopment.

This story of change pulls out the key findings and recommendations from EMERGE case study 6, which focuses on the One Man Can initiative in South Africa. The initiative works through community mobilisation to question gender norms and improve knowledge and practices around sexual and reproductive health.

This story of change pulls out the key findings and recommendations from EMERGE case study 3, which focuses on the work of KMG to eliminate female genital mutilation-cutting in Ethiopia.

Against the context of underlying poverty, HIV/AIDS and an over-stretched and underresourced education system, many children in Malawi have reduced and sporadic access to schooling and are at risk of permanent dropout. Evidence from the sub-Saharan Africa(SSA) region suggests that a disproportionate number of marginalised children are those orphaned and made vulnerable by HIV/AIDS. International goals for Education for All (EFA) will not be realised unless education systems can reach out to and retain these children. More needs to be done in schools to address their specific needs and support their access to learning. Acknowledging this, there is a growing call for conventional primary schooling to become more open, flexible and inclusive.This report introduces a model of education that uses open, distance and flexible learning (ODFL) to strengthen and support access to learning within conventional schools.
The model utilises low-tech ODFL strategies –

Global health and poverty reduction discourses have recognised immunisation as one of the most affordable and effective means of reducing child mortality and in a broader sense, as an essential contribution to poverty reduction efforts. While immunisation comes with countless benefits, it is potentially a complex and difficult health strategy to enforce. Decisions on broader health as well as immunisation goals are often made at a global level to be incorporated and adapted in to national health plans and budgets. Evidently for immunisation campaigns, the journey from the global to the local is a vulnerable and unpredictable one. Indeed ‘anti-vaccination rumours’ have been defined as a major threat to achieving vaccine coverage goals. This is demonstrated in this paper through a case study of responses to the Global Polio Eradication Campaign (GPEI) in northern Nigeria where Muslim leaders ordered the boycott of the Oral Polio Vaccine (OPV).

This paper examines the evidence on access to conventional schooling for children and young people affected by HIV and AIDS in sub-Saharan Africa and makes recommendations for the further development of the SOFIE Project. The findings reveal the highly complex and context specific nature of the educational impact. In some areas broad adaptive capacities are emerging that may enable households to support a larger number of orphans whilst in other areas households are reaching the limits of their capacity to cope. In HIV-stressed households children have reduced educational access and attainment and maternal orphans are a particularly disadvantaged group in terms of schooling, even relative to other poor children. At the same time schools in high HIV prevalence areas are increasingly challenged to meet the educational and emotional needs of the children who walk in through their door and are unlikely to reach out to the young people who cannot attend regularly.

Infant immunisation is currently a focus of national and global policy attention in relation to Africa as a key means to address ill-health and contribute to the Millennium Development Goals. Yet vaccination coverage is stagnant or falling in many African countries. Redressing such declines, and ensuring the effectiveness and sustainability of proposed expansion of immunisation programmes, requires a sound understanding of the factors shaping vaccine delivery and acceptance in contemporary African health systems. This paper explores these issues through an anthropological approach.

This paper examines public engagement with routine vaccination delivery, and vaccine trials and related medical research, in The Gambia. Its approach is rooted in social and medical anthropology and ethnographic methods, but combines insights from the sociology of scientific knowledge, and ‘actor-oriented” sociology in development. Current analysis and professional reflection on public engagement with vaccination reflects the concepts and imperatives of health-providing and research institutions. In contrast Gambian parents’ perspectives are couched in very different conceptual and experiential terms, linked to the wider dilemmas of raising infants in a hazardous world. In this context the paper traces parents’ experiences of routine infant welfare clinics and then how they narrate their experiences with two vaccine related studies orchestrated by the Medical Research Council laboratories.
A range of contrasts emerges. Whereas health professionals tend to attribute vaccination acceptance to the acquisition of modern scientific attitudes,

This paper examines the controversy over measles, mumps and rubella (MMR) vaccine in Britain through the lenses of social movement theory and social studies of science. Since the early 1990s, networks of parents have raised, and mobilised around, concerns that MMR has triggered a particular disease in their children linked to autism and bowel problems, and have been supported in this by certain scientists. In the high-profile and highly-public debate which has ensued, they have challenged established perspectives and institutions in both biomedical science, and public health policy. While much policy and public debate has dismissed their concerns as based on emotion, misinformation or “junk science”, this paper locates them as part of a citizen science grounded in parental experience.
It tracks how the framing and strategies of parental mobilisation around MMR have developed, in relation to a growing counter-mobilisation from scientists,

Political impact and implications: Initial analysis suggests that governments’ poor management of the Ebola crisis has generated frustrations and exposed citizens’ lack of trust in their governments. The Ebola crisis is likely to play a very political role in the next election in Sierra Leone and there are predictions that the opposition will win as a result. Economic impact and implications: The economic impact of the Ebola crisis includes loss of gross domestic output, threat to food security, fall in employment and livelihoods, and decline in foreign investment. Growth has slowed in Sierra Leone and is likely to fall even further. Household income has fallen, financial reserves are being used up and large numbers of people are now food insecure. Some businesses are benefiting from the local procurement by the international Ebola response.
Social impact and implications: Progress in human development is likely to be reversed due to the impact of the Ebola crisis on health,

This report focuses on vulnerable groups in Burma and access to basic services. The first part of the report outlines groups considered to be vulnerable and marginalised. These include minority ethnic groups (such as the Chin, Kachin, Karen, Karenni, Mon, Rohingyas, Shan). In some cases, minorities’ ethnic identity is closely linked with a religion other than the majority Buddhism. Other vulnerable groups are internally displaced persons (IDPs); women and girls; and children generally. Intersectionality of these identities can exacerbate vulnerability. For example, minority ethnic groups often live in conflict zones or areas with government authorised development projects.
They are thus more likely to suffer from internal displacement, which brings additional challenges and insecurities. Additionally, women and girls from ethnic minority groups may be specifically targeted by armed forces and become victims of sexual violence.The second part of the report discusses barriers to accessing basic services,

There appears to be very little literature on the effectiveness of non-state providers (NSPs) of health services in fragile states. There is some useful case study material, particularly from Afghanistan and Cambodia although this tends to focus on the effectiveness of service provision rather than the extent to which NSPs align services with government systems and policies. Furthermore, there is no consensus on what actually constitutes ‘effectiveness’. Antuono et al (2006) evaluate the involvement of NGOs in service delivery in Bangladesh and Nepal in terms of effectiveness, cost, accountability and transparency, sustainability and transferability.
In most cases however, the literature offers no such clarification. Notwithstanding these limitations, this helpdesk report: presents literature on non-state provision of health services1 in fragile, conflictaffected, and post conflict states, including a number of country case studies; and explores the issue of effectiveness of non-state providers in low income countries in general.
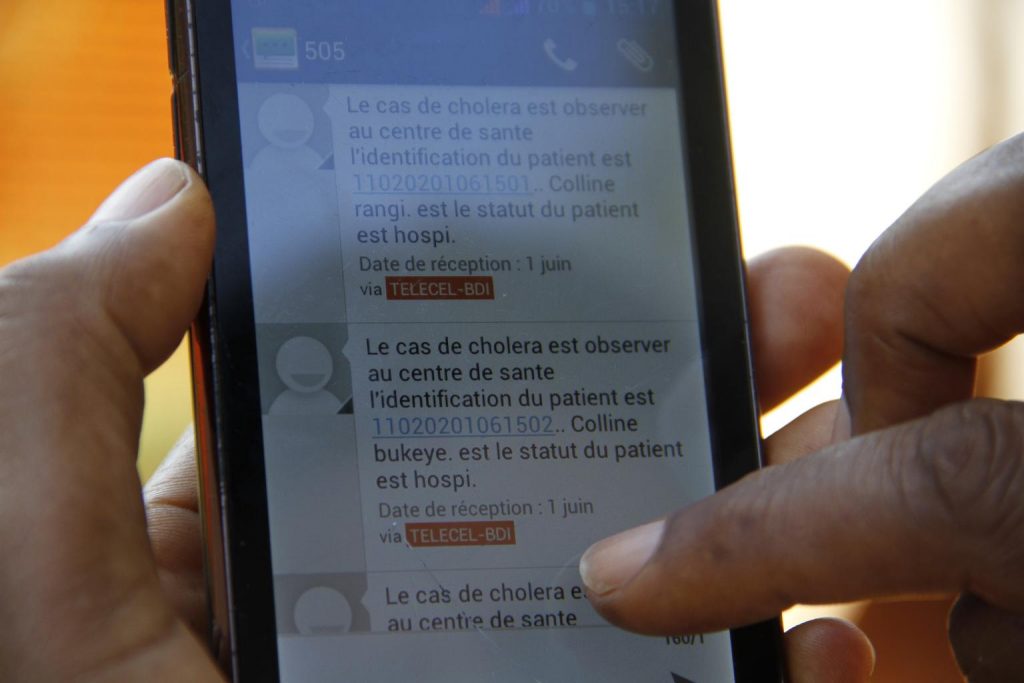
This report provides some recent examples of the use of mobile telephony to improve health serviceoutcomes. There is significant potential for the use of mobile telephony to improve health serviceoutcomes and data management.
Opportunities include: serving as a less costly substitute for existinginterventions; providing interactive functions that multiply the power of existing interventions; andserving entirely new functions.

Global risks of zoonotic disease are high on policy agendas. Increasingly, Africa is seen as a ‘hotspot’, with likely disease spillovers from animals to humans. This paper explores the social dynamics of disease exposure, demonstrating how risks are not generalised, but are related to occupation, gender, class and other dimensions of social difference.
The Community Led Ebola Action (CLEA) has empowered communities to do their own analysis and take their own action to become Ebola-free in Sierra Leone. CLEA has focused on triggering collective action by inspiring communities to understand the urgency and the steps they take to protect themselves from Ebola. Community Mobilisers have facilitated this process and communities have modified norms, beliefs and behaviours in response to the conditions around them.
The CLEA Approach was used to trigger 9,285 communities in Sierra Leone as of April 2015. 100% of these communities developed action plans and these were followed up by more than 50,000 individual community visits by SMAC-trained Community Mobilisers. Significant reduction in unsafe burials and people with symptoms reporting within 24 hours were recorded over the course of these visits.
CLEA draws on successful examples of community participation and the use of Participatory Rural Appraisal in HIV and AIDS and other health programming.
The CLEME (Community Led Ebola Man- agement and Eradication) programme aims at triggering the behavioural change needed by the communities to strengthen community resilience to the outbreak and prevent further resurgence by ensuring real and sustainable improvements through:
Providing the communities with the means to conduct their own appraisal and analysis of the Ebola outbreak, their safety regarding the disease and its con- sequence if nothing is done;
Instilling a feeling of urgency in engaging in community actions that will prevent the community experiencing infections;
Supporting technically the communities in the implementation of the identified solutions and actions adopted.
CLEME (Community Led Ebola Management and Eradication) is an approach developed under the initiative of Action Contre la Faim (ACF) Sierra Leone hygiene promotion field teams, at the start of the Ebola outbreak, based on extensive experience with the Community Led Total Sanitation (CLTS) approach.
Ebola Virus Disease (EVD) home deaths occur as the result of infected persons not being detected early and sent to Ebola Treatment Units (ETU) where they can access care and have an improved chance of survival. From a public health standpoint, EVD deaths should not occur at home. Individuals suspected of being infected with EVD should be identified through case investigations or contact tracing efforts and then referred to an ETU, thus decreasing their risk of dying as well as minimising the risk of exposing others to the disease.
This report presents results of a rapid anthropological assessment conducted in response to a request from the U.S. Centers for Disease Control and Prevention’s (CDC) Epidemiology Team in Monrovia in December 2014 for qualitative data to better understand why EVD deaths were occurring at home in urban Montserrado County. Data from the International Federation of Red Cross and Red Crescent Societies (IFRC) had indicated that 30% of the 60-90 deceased persons collected weekly from ETUs and community settings in Monrovia by Liberian Red Cross burial teams between early November and early December had tested positive for EVD and nearly half of those had been collected in homes.This raised concerns that EVD case-finding and prevention efforts were not as effective as they could be.