
The world’s highest HIV prevalence and the increasing number of deaths due to AIDS is having unprecedented impact on Swaziland. Worryingly, with a generation of orphans and rapidly escalating poverty, this desperate situation is being accepted as ‘normal’. HIV/AIDS in Swaziland has been characterized by a slow onset of impacts that have failed to command an emergency response.With insufficient resource allocation and a lack of capacity, slow onset events can become emergencies.The absence of an agreed definition of “disaster” or “emergency” has helped to sustain this characterisation.
The nature of these terms is changing.The case of Swaziland emphasizes that they can be long- term, complex, widespread events that evolve over years.Allocating humanitarian funding according to need is important. The current paradigm of emergencies is inadequate for assessing situations that develop slowly and quietly. There is broad agreement within humanitarianism that reflects a concern with reducing suffering and preserving human dignity.

This After Action Review (AAR) covered CARE’s responses to the Cholera Crisis in Zimbabwe from 2008 to 2009. The purpose of this AAR is to contribute to CARE’s understanding of the cholera response, and to help promote learning and accountability throughout CARE International.
This report contains a brief overview of CARE’s emergency response activities; a debate of the workshop methodology and process; and the relevant lessons learned and recommendations identified.

The purpose of this public health risk assessment is to provide health professionals in United Nations agencies, nongovernmental organizations, international and local organizations, donor agencies and local authorities, who are currently working with populations affected by the emergency in the Horn of Africa,with up-to-date technical guidance on the major public health threats faced by the populations affected by the drought and famine conditions in the sub-region.
The topic areas addressed have been selected on the basis of the burden of morbidity and mortality, as well as the potential for their increased risk in the affected area. Public health threats represent a significant challenge to those providing health-care services in this evolving situation. It is hoped that this risk assessment will facilitate the coordination of activities between all agencies working among the populations currently affected by the crisis

In 2012 Uganda experienced many disease outbreaks including Measles, Ebola, Marburg and Nodding disease. Two Ebola outbreaks and one Marburg event were in quick succession and placed the Ministry of Health and the Uganda Red Cross (URCS) as well as other partners under significant pressure to respond to one of the world’s deadliest diseases in three separate locations.
The objectives of the evaluation included: 1. Review current operating procedures of URCS’ epidemic response including the roles and responsibilities of URCS in relation to MoH, WHO and other partners as well as internal structures for coordination and integrations of activities across departments. 2. Review the operational effectiveness and accountability of the response against planned outcomes and the use of DREF funds against proposed activities 3. Evaluate the response of URCS to epidemics, against the needs of beneficiaries and communities focused on the areas of most ‘added value’ of the URCS;
In recent months Uganda has experienced three separate Viral Hemorrhagic Fever (VHF) outbreaks. Two Ebola outbreaks in the districts of Kibaale and Luwero and one Marburg event in Kabaale. URCS responded in all three cases with assistance from the IFRC Disaster Relief Emergency Fund (DREF) and aimed to support clinical interventions from the Ministry of Health (MoH) and Medicins Sans Frontiers (MSF). In order to fully explore the value added of Psychosocial Support (PSS) and community based volunteers in this type of epidemic response, the unique opportunity of these outbreaks was utilized to document and learn from.
Three independent evaluators representing Disaster Management, Health and Psychosocial support were sent to the affected areas in February of 2013 to gather lessons learned of the response. The main aim of this assessment was to evaluate the PSS response of URCS to these VHF,

This report examines the sharp rise in inequality in Malawi between 2004/5 and 2010/11, and models the link between poverty, inequality and growth from 2015 to 2020.

This rapid review explores the impact of protracted crises on attitudes and aspirations. It provides a general overview of what is meant by the term protracted crisis, a broad reading of the influence of different types of protracted crisis on attitudes and aspirations and a review of literature that discusses the impact of protracted crisis in Karamoja and on Karamojong attitudes and aspirations.
The review draws on both academic and grey literature, which reflects the variety of approaches to understanding attitudes and aspirations and how they are formed. Of particular importance are discussions of social norms, networks and capital and how these shape relations between individuals and groups and thus influence the formation and evolution of attitudes and aspirations.

An ACAPS Briefing Note on crisis in Somalia.

An ACAPS Briefing note on the worst drought in Ethiopia for 50 years.

Resistance to the Ebola response has been more widespread and more severe in Guinea, than in Liberia and Sierra Leone, with sometimes violent incidents.
This is due to a complex interaction of many factors, including underlying causes and the nature of the response.

This document uses lessons learned from recent coordinated assessments to distil key points,advice, and pitfalls in carrying out a Coordinated Assessment during the first weeks of a disaster. It provides a general introduction to what has been learned about coordinated assessments in terms of what works and what does not.
As such, it is aimed towards humanitarian personnel responding to or preparing for emergencies both at field and headquarters level.
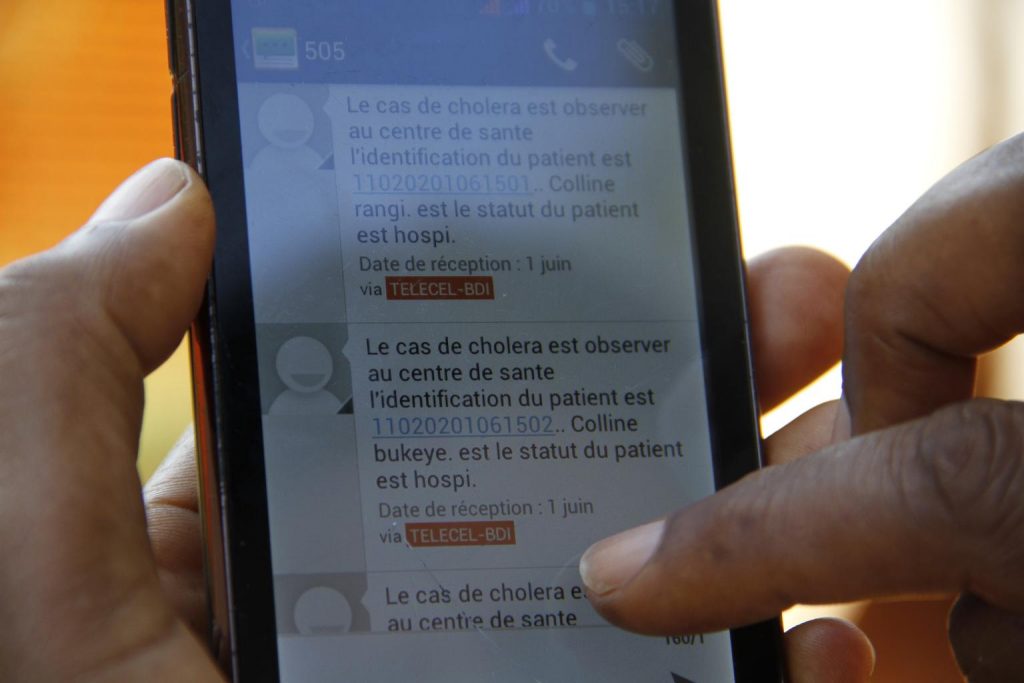
Information about the displacement of people after disasters is crucial in determining the scale and impact of the emergency, and is vital for conducting humanitarian needs assessment on the ground. Methods to forecast or detect such migration are however very limited at present. The use of geo-referenced mobile phone call data to understand post-disaster movements of affected people has been demonstrated in two studies, in the aftermath of the Haiti (2010) and Christchurch, New Zealand (2011) earthquakes.
These studies, matched against aid agencies’ recurring information needs in disaster response operations, suggest that this type of data has potential to be a useful new method to forecast and locate people who have been displaced and therefore in need.

A scenario projects alternative ways in which a situation might evolve. It is a set of informed assumptions about a situation that may require humanitarian action. Building scenarios involves speculating about an uncertain future and envisaging different possible outcomes for a given initial situation.
When applied to the framework of a needs assessment,scenarios are used to plan for possible future humanitarian crises and needs.

The objective of this technical brief is to provide guidance on how you could assess the quality of information used as evidence for decision making during humanitarian needs assessments. It aims to assist analysts in understanding the distinction between sources and information, assessing the quality of different data types (primary and secondary data), and using appropriate criteria for judging information generated through quantitative or qualitative research methods.
It suggests way sof dealing with inconsistent information and offers advice on how to use evidence, establish confidence in findings and, communicate uncertainty.

This Technical Brief is for assessment experts, information management officers and information analysts planning or implementing assessments in emergency contexts. It provides guidance on how to select and use suitable methods when conducting a population estimation exercise.This technical brief builds upon the desk review Rapid estimation of affected population figures, which has identified and detailed a broad range of different population estimation methods.
These methods are categorised by sampling methods, site estimation methods,counting methods, remote estimation methods and the usage of existing demographic data. It is recommended to use the above mentioned review as a reference for more in-depth information about the different techniques described in the present document. The present technical brief should be considered as a companion to the review.

Humanitarian needs assessments are carried out to determine the immediate needs of a population following an emergency or humanitarian crises.
Once an assessment has been carried out and data has been analysed, humanitarian organisations can make key decisions about their operational response including their goals, intended programmes and fundraising plans.

The aim of these guidelines is to describe the systematic development of an SDR during the initial days and weeks after a disaster.
It is based on ACAPS’ experience in developingSecondary Data Reviews for a number of Sudden Onset Disasters over three years.

The purpose of this technical brief is to assist humanitarian workers in using secondary demographic data in emergencies. It recommends building a context specific demographic profile based on available information. It proposes some rule-of-thumb standards, which can be adapted to the local context, tailoring to the purpose and the time available.
The document provides: 1. Long term guidance sheets (if you have a few days): identifying demographic ‘mega trends’, and possible interactions with disaster risk, impact and response. This broader perspective is essential for interpreting data in emergencies, and as input for longer term strategy (e.g. CAP orSRP) 2. Short term quick start (if you have an hour):accessing demographic data for immediate operational needs in a specific emergency,such as input in a flash appeal (e.g. within24-48 hours).Clearly, this supplements, rather than replaces,the need for primary data, but is intended to be helpful in preparing for large scale primary data collection,

This Technical Brief is intended to be a starting point for improving coordinated needs assessments in urban areas, without which the humanitarian community will not be able to ensure the quality and accountability of urban response itself. It provides guidance on carrying out joint rapid assessments of humanitarian needs in urban environments within the first weeks of a disaster.
Organisations can use this Brief to ensure that joint assessments are carried out appropriately in urban areas, and to update their assessment practice. The Brief does not cover more comprehensive or in-depth sectoral assessments that may take place in the longer-term, although the issues discussed are the same and many of the principles are still applicable. It does not provide sector-specific guidance, and does not focus on the needs of specific groups (such as women or the elderly),but it does list references and resources that provide this detail.

Monitoring of social media conversations in the aftermath of the Nepal earthquake was found mainly to be useful in two ways:
1. Analysing public reactions to media reports: The data enabled the team and clients to see which issues were widely discussed, and whether these conversations led to sustained discussion or merely short-term spikes. (See detailed example in Annex 1.)
2. Seeing the relative prevalence of topics and identifying changes: Where a pure quantitative analysis can only show that a certain area of discussion is gaining or losing volume, a qualitative analysis was able to identify which sub-topics gained importance. For example, a shift in conversation from response-related topics towards reconstruction.

The brief starts with an explanation of the main purpose of a questionnaire and the principles that should be followed to reach these objectives. Afterwards, the ten steps of questionnaire development are discussed. The brief concludes with sections on what to keep in mind specifically when designing a questionnaire and individual questions. It focuses on questionnaire design for interviewer administered (as opposed to self-administered) surveys, as this is the most common approach used in humanitarian emergencies. However, Section two briefly touches upon the impact of different survey modes on questionnaire format and wording.
This brief focuses on how to gather the information required; it does not provide recommendations on what information should be collected. In addition, the design, roll-out and ultimately the success of an assessment involves much more than designing a questionnaire. It includes deciding the sampling strategy, arranging logistics,

Severity is a key parameter in humanitarian decision making. “Severe” is part of ordinary language; “severity” more institutional. We make absolute statements (“The patient is in asevere condition”) as well as comparative ones (“The townspeople are even more severely impacted than the farmers”). The bases of such judgments are not always clear. By contrast,needs assessments in humanitarian action strive to define severity measures that are transparent, tightly related to needs concepts, and fit to support valid comparisons.The function of severity measures is to substantiate priorities that, together with parameters like access and cost, guide decisions on the humanitarian response. Severity measures condense, in one number or one verbal scale, elements that influence judgments on priority – elements that are conceptually different, or arrive from separate information sources.
Such constructs have been around for several decades, at first in public health.The humanitarian community developed its own gradually,

The humanitarian community often finds itself unprepared for unfolding humanitarian developments or sudden events: the 2010 cholera outbreak in Haiti and the sudden spread of Islamic State areas of control in 2013 in Syria are just two of the many examples. Scenario building, an analysis of how situations might evolve, is an essential part of humanitarian operations as it informs contingency planning and preparedness measures ahead of possible developments. It can also help to ensure programming is sufficiently robust to withstand changes in the operational environment. During a separate contingency planning exercise, appropriate preparedness measures and detailed response plans are developed, based on the existing and possible future capacity to respond to the identified scenarios.
During scenario building the range of plausible developments, their predicted impact on the people affected, and the related needs are identified. Scenario building covers a range of activities including:o Risk analysis: the identification and impact of a probability of damage,

A report prepared to inform DFID on the strengths and weaknesses of the current global health architecture, and of the relevance and responsive of the health architecture for the post 2015 agenda.

The Ebola outbreak currently affecting West Africa is the most serious trans-national medical emergency in modern times. It has the potential to become a global health crisis. Many of the countries affected already have weak health systems, which are now stretched to breaking point. The health authorities have a limited capacity to respond and in a context of widespread fear and misunderstanding about the nature of the disease and how to prevent it.
Alongside addressing human resourcing, health system and pharmaceutical challenges, social mobilisation is increasingly recognised as a key component of any strategy that aims to bring the Ebola outbreak under control. This helpdesk seeks to establish what lessons have been learnt from the current and previous Ebola outbreaks. It recommends good practice and makes suggestions based on the evidence for good practice and preparedness to reduce transmission and prevent further risk and exposure in affected countries.

This helpdesk focuses on the impact of traditional healers, witch doctors and burial attendants on ebola in West Africa. It seeks to establish if there is a difference between witch doctors, herbalists and traditional healers in terms of when people see them and the kind of treatment they provide.
It goes on to explore the roles of these actors in preparing bodies for burial and at funerals. It provides information on secret societies. The report goes on to explore behaviour change. It provides information on payment of traditional healers as a leverage point.

The purpose of the review was to provide a summary of possible indicators which might be used to measure the performance and quality of healthcare in conflict-affected settings.
There is considerable guidance on measuring access, availability and quantity of health provision in these settings, but much less on whether this care is sufficient or effective. This
review identifies and summarises some indicators which have been used or are suggested as appropriate.

Syria’s shattered health system is forcing health workers to engage in brutal medical practices and a series of epidemics have left millions of children exposed to a plethora of deadly diseases. This report sheds light on a broken health system and its consequences: children not just dying from violent means but from diseases that would previously either have been treatable or prevented.
The extent of the health system collapse in Syria is borne out in many horrific ways, including: Children having limbs amputated because clinics don’t have necessary equipment for appropriate treatment, Newborn babies dying in their incubators during power cuts, Patients being knocked out with metal bars owing to a lack of anaesthesia, Patients undergoing potentially deadly person-to-person blood transfusions.

The Ebola epidemic ravaging parts of West Africa is the most severe acute public health emergency seen in modern times. Never before in recorded history has a biosafety level four pathogen infected so many people so quickly, over such a broad geographical area, for so long’ (Margaret Chan, 26th September 2014, WHO).This report focuses on the local beliefs and practices around illnesses and death, the transmission of disease and spirituality, which affect decision-making around health-seeking behaviour, caring for relatives and the nature of burials. It also considers how this can inform effective behaviour change interventions for preventing Ebola in Sierra Leone. Four key transmission pathways are considered; unsafe burial, not presenting early, care at home and visiting traditional healers.Indigenous beliefs and responses to Ebola are rarely mentioned and when they are images of ignorance, exoticism and superstition are what prevail (Hewlett and Hewlett 2008).

Diseases such as Ebola highlight the importance of a holistic focus on health systems, as opposed to assuming that health is the preserve and concern of health professionals alone. This was the lesson Uganda learnt very quickly in managing the Ebola outbreak in 2001.
Until the current epidemic in West Africa, Uganda held the unfortunate record for the greatest number of infections, with 425 recorded cases of Ebola, of which 224 people sadly died.

The world is becoming more urban every day, and the process has been ongoing since the industrial revolution in the 18th century. The United Nations now estimates that 3.9 billion people live in urban centres. The rapid influx of residents is however not universal and the developed countries are already urban, but the big rise in urban population in the next 30 years is expected to be in Asia and Africa.
Urbanisation leads to many challenges for global health and the epidemiology of infectious diseases. New megacities can be incubators for new epidemics, and zoonotic diseases can spread in a more rapid manner and become worldwide threats. Adequate city planning and surveillance can be powerful tools to improve the global health and decrease the burden of communicable diseases.

The effects of armed conflict and natural disasters on global public health are widespread. Much progress has been made in the technical quality, normative coherence, and efficiency of the health care response. But action after the fact remains insufficient. In the years ahead, the international community must address the root causes of these crises. Natural disasters, particularly floods and storms, will become more frequent and severe because of climate change.
Organised deadly onslaughts against civilian populations will continue, fueled by the availability of small arms, persistent social and political inequities, and, increasingly, by a struggle for natural resources. These events affect the mortality, morbidity, and well-being of large populations. Humanitarian relief will always be required, and there is a demonstrable need, as in other areas of global health, to place greater emphasis on prevention and mitigation
Ebola is just one of the many crises the world faced through 2015, which also saw the Nepal earthquakes, Yemen civil war, South Sudan conflict and the Syrian refugee crisis to name but a few.
So, what have we learnt? What is the most effective way of rebuilding a country after catastrophe?

Of the 46 countries in the World Health Organization (WHO) African region (AFRO), 43 are implementing Integrated Disease Surveillance and Response (IDSR) guidelines to improve their abilities to detect, confirm, and respond to high priority communicable and non-communicable diseases. IDSR provides a framework for strengthening the surveillance, response, and laboratory core capacities required by the revised International Health Regulations (IHR, 2005)]. In turn, IHR obligations can serve as a driving force to sustain national commitments to IDSR strategies.
The ability to report potential public health events of international concern according to IHR (2005) relies on early warning systems founded in national surveillance capacities. Public health events reported through IDSR to the WHO Emergency Management System in Africa illustrate the growing capacities in African countries to detect, assess, and report infectious and noninfectious threats to public health. The IHR (2005) provide an opportunity to continue strengthening national IDSR systems so they can characterise outbreaks and respond to public health events in the region.

With more than 3000 deaths since the first case was confirmed in March, 2014, the international community has recognised Ebola as a public health emergency of international concern and a clear threat to global health security. It is the subject of a high-level UN Security Council resolution, and has triggered the creation of a UN Mission for Ebola Emergency Response.
The International Health Regulations (IHR) represent the system designed to prevent national public health emergencies from becoming international crises. WHO’s historic responsibility has been to control the spread of disease. The IHR were adopted in 1969 (IHR 1969). In 1995, in the wake of plague in India and Ebola in DR Congo, a resolution was passed in the World Health Assembly (WHA) to revise and update the IHR.

This spring, when the team from the Ebola Response Anthropology Platform evaluated Community-Based Ebola Care Centres (CCCs) in Sierra Leone, one thing they constantly heard complaints about was human-resource management. Residents of the communities where the Centres were located grumbled about favouritism: well-paying jobs in the Centres were given to friends and family of the local paramount chiefs. Local health authorities questioned the medical competency of CCC staff. Staff in primary health units complained about unequal pay and benefits. They focused on the views on the development, implementation and relevance of the CCCs from the perspective of the communities next to and near where they were located.
Meanwhile, a different evaluation team which focused on the quality of care in the Centres was coming to a very different conclusion. They did report that the Ministry of Health and Sanitation, implementing partners,
