
Female genital mutilation (FGM) is a deeply entrenched cultural practice involving the partial or total removal of the external female genitalia for non-medical reasons. It is recognised as a severe violation of human rights. Worldwide, four million girls are subjected to this practice each year, with four in ten FGM survivors living in fragile and conflict-affected countries.1 The practice of FGM is addressed in UN Sustainable Development Goal 5.3. This goal aims to eliminate all harmful practices including FGM and child, early, and forced marriage by 2030 – including among those living in crisis-affected areas and/or those forcibly displaced. Countries hosting refugees, asylum-seekers and other migrants must ensure that national strategies to address FGM are relevant and appropriate to the diverse populations that countries have a responsibility to protect. These strategies must also consider additional vulnerabilities such populations may have, related to conflict and displacement.
This SSHAP Brief focuses on the context of FGM for Sudanese populations in Egypt who currently make up the largest group of forcibly displaced people (refugees, asylum-seekers and undocumented migrants) there since the escalation of armed conflict in Sudan in April 2023. Both Egypt and Sudan have some of the highest rates of FGM in the world. This brief reviews the FGM context and anti-FGM programming developments in both countries. It considers the drivers and dynamics of FGM practices in the context of forced displacement to inform culturally sensitive strategies for FGM prevention and response for forcibly displaced Sudanese people in Egypt. It draws on academic and grey literature as well as consultations with experts working with affected populations in Egypt.
Key considerations
- Encourage the respectful framing of FGM as a cultural practice. Displaced people from diverse backgrounds, such as Sudanese communities, already face discrimination in Egypt. Framing FGM negatively risks deepening their sense of alienation and unacceptance. A more culturally sensitive approach acknowledges the diversity within their cultural practices. Engaging these communities collaboratively in the messaging on FGM helps build trust and positions them as key allies in efforts to abandon this harmful practice.
- Work across disciplines and sectors to address the multidimensional impacts of FGM. Highlighting the multidimensional consequences of FGM underscores the necessity for a multisectoral and comprehensive approach to address its far-reaching impacts. These include physical and psychosocial complications, which can be chronic or even fatal.
- Address the forced displacement journey and its impact on women and girls. The displacement journey is marked by intersecting experiences of violence; for women and girls who have already undergone FGM, this can exacerbate both medical and psychological complications. FGM programming must be mindful of these vulnerabilities, ensuring that support services address the compounded effects of displacement, violence and FGM.
- Cultivate culturally sensitive partnerships utilising local knowledge. Organisations aiming to promote FGM abandonment in Sudanese displaced populations should consider partnering with Sudanese civil society, women-led groups, grassroots organisations and local activists with experience in resisting the practice. These partners are better equipped to understand the cultural and social norms that sustain FGM, and their trust within communities makes them ideal collaborators. Drawing on initiatives such as Sudan’s anti-FGM campaign, ‘Saleema’, can complement ongoing efforts and ensure culturally relevant programming for displaced Sudanese populations.
- Champion child-centred approaches to FGM through community-led schools. Collaborating with Sudanese-led community schools and nurseries can provide a unique opportunity to reach displaced children with tailored anti-FGM messages. Many of these children – especially those who are unregistered and are excluded from formal education – remain at risk. Reaching them through trusted institutions helps ensure interventions engage vulnerable populations effectively.
- Empower displaced workers in FGM abandonment efforts. Strengthening the capacity of displaced workers to discuss the long-term impact of FGM is essential. Programmes should provide displaced workers with the knowledge and tools they need to confidently and sensitively engage their communities on this topic, while also recognising the complexity of personal circumstances and relationships.
- Build the capacity of midwives and traditional circumcisers as change agents. Sudanese midwives and circumcisers often have significant influence in their communities. Nevertheless, when professional midwives refuse to perform FGM, some families resistant to change may seek out traditional midwives for FGM and other childbirth services. This puts pregnant girls and women at greater risk of obstetric complications. Programmes should work with both professional and traditional midwives to manage and refer FGM-related medical complications, particularly those resulting from Type 3 FGM.
- Push economic empowerment as a strategy for FGM prevention. Many forcibly displaced people in Egypt lack economic empowerment, limiting their ability to resist harmful practices like FGM. Integrating livelihood programmes and vocational training into FGM and gender-based violence (GBV) interventions can empower survivors and support awareness-raising efforts. Special attention should be given to traditional circumcisers, who may face economic pressure to continue practicing FGM. Offering alternative income-generating opportunities can help them transition away from this harmful practice.
- Contextualise FGM interventions to meet displaced people’s needs. Recognising the diversity of Sudanese communities is essential for understanding FGM behaviours and attitudes. Displaced communities vary in their adherence to FGM, and programming must be tailored to reflect these differences. Collaborating with displaced people as change agents within their communities has proven effective in identifying girls at risk of FGM and responding to specific community needs.
- Ensure programme design is informed by research and anchored in evidence. There is an urgent need for research on how FGM practices and attitudes are evolving among different Sudanese and displaced populations in Egypt. This evidence will allow responding agencies to design protection strategies that are both effective and context specific. Research should consider co-production principles, involving displaced people as co-researchers, to ensure the empowerment of women and the displaced community.
- Engage communities in FGM prevention in an inclusive way. FGM interventions should engage all members of the displaced community, including men and boys. Their involvement is crucial to fostering a multisectoral approach that addresses the broader social dynamics sustaining FGM. Engaging men and boys in anti-FGM efforts can leverage their social influence, helping to share the responsibility of abandoning this practice.
Types of FGM and their impact
FGM is defined by the World Health Organization (WHO) as ‘all procedures involving partial or total removal of the external female genitalia, or other injuries to the female genital organs for non-medical reasons.’2 Other ways FGM is referred to include ‘female genital cutting’ and ‘female circumcision’. There are no health benefits to FGM. Women and girls who undergo FGM suffer from a spectrum of short through to long-term physical and psychosocial complications. Physical complications include pain, reduced sexual enjoyment, menstrual problems, and chronic infections; psychosocial complications include trauma, anxiety, depression, stigma and low self-esteem.3 These consequences depend on the type of FGM and the conditions under which the procedure was performed.
WHO categorises FGM into four types, as follows: Type 1 – partial or total removal of the clitoris and/or the prepuce; Type 2 – partial or total removal of the clitoris and labia minora, with or without excision of the labia majora; Type 3 – narrowing of the vaginal orifice by cutting and bringing together the labia minora and/or the labia majora to create a seal, with or without excision of the clitoris (in most instances the cut edges of the labia are stitched together, which is referred to as ‘infibulation’); and Type 4 – all other harmful procedures to the female genitalia for non-medical purposes, e.g., pricking, piercing, incising, scraping and cauterisation.4
In addition to the medical classifications of FGM types, popular classifications, which reflect historical and social contexts, may differ from one country to another and between communities within the same country. Common terms to refer to FGM in Egypt include ‘tahara’ (meaning ‘purification’); ‘khitan’ (meaning ‘circumcision’); ‘khafd’ (meaning ‘reduction or lowering’); and the ‘Sunna’ cut (with Sunna, meaning ‘path or way’, referring to actions underpinning Islamic teachings – this is now usually described as a misinterpretation of Islamic practice). All of these terms tend to refer to the medical FGM Type 1 and 2. Egyptians also use the term, ‘khitan sudani’ (Sudanese FGM) to refer to the infibulation Type 3 of FGM common in Sudan. Among Sudanese people, the term ‘tohoor’ (‘purification’) is generally used and Sunna is also commonly used for Type 1 and 2. Type 3 is commonly called ‘fir’auni’ (‘pharaonic’) FGM. This references the practice’s origins from ancient Egypt when female circumcision was practiced as a way to detach a woman from her masculine soul – as theorised by historians.5,6
Findings from studies of FGM in multiple displacement settings suggest that girls and women who have undergone FGM have complex medical and psychosocial needs relating to their intersecting experiences of violence.7 Consequences range from less specific references to extreme emotional distress, including anxiety and depression. Different manifestations of trauma reflect traumas that occurred throughout the migration journey; age at the time of FGM; and discussion about the practice before the cutting occurred. Some Sudanese survivors of FGM in Egypt may similarly be expected to face challenges related to socialisation, suicidal ideation, and negative coping strategies including substance misuse.
Context of FGM in Egypt
The practice of FGM was made illegal in Egypt in 2008 and rates are declining. However, Egypt still has one of the highest FGM rates globally. In 2021, 86% of women and girls aged 15 to 49 who had ever been married had undergone FGM, with Type 1 and 2 predominating.8 The practice is declining in younger generations; among girls aged 15 to 17, the prevalence of FGM dropped from 61% in 20149 to 37% in 2021.8
Attitudes are shifting as well, with the proportion of women supporting FGM falling from 75% in 200010 to 30% in 2021.8 Additionally, only 25% of women in 2021 believed men wanted the practice to continue, compared to 50% in 2014.8,9 However, seven million girls were projected to remain at risk of undergoing FGM between 2015 and 2030. Progress on abandoning FGM must be 15 times faster for Egypt to meet the SDG target and eliminate FGM by 2030.11
Figure 1 shows the prevalence of FGM across different governorates in Egypt. In Lower Egypt, the prevalence among women aged 15-49 ranges from 80% in Cairo and 86% in Giza to about 70% in Alexandria – cities that serve as major hubs for displaced people. In contrast, Upper Egypt exhibits a significantly higher prevalence rate of 98% – particularly in Aswan (spelled ‘Assouan’ in Figure 1).
Figure 1. Heat map showing FGM prevalence in women (15-49) by governorate in Egypt
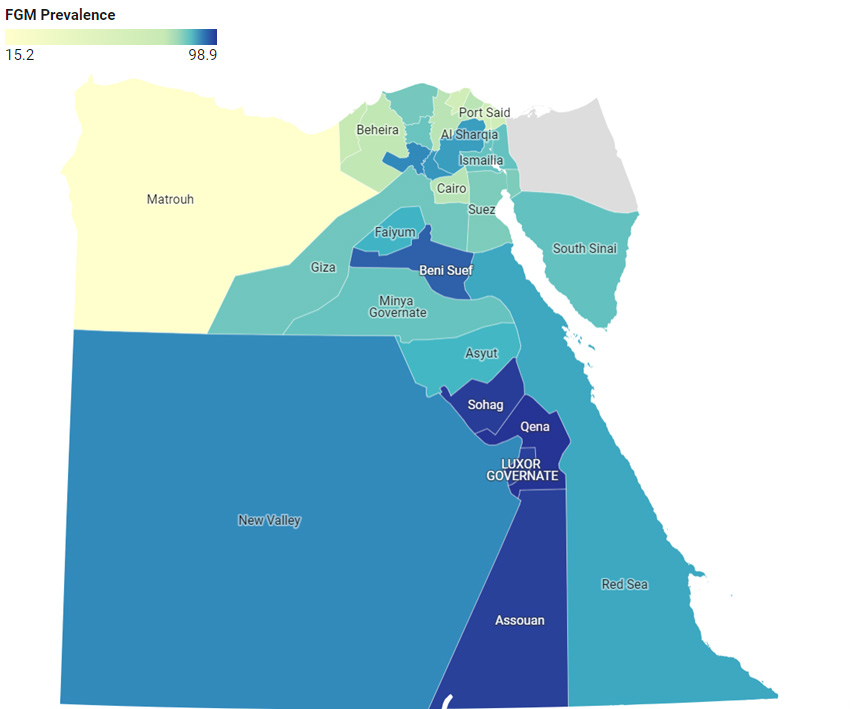
Source: Author’s own. Created using Datawrapper. Calculations based on the Egyptian Family Health Survey (2021).8
Drivers and risk factors for FGM in Egypt
Despite these positive trends, significant challenges to eradicating FGM remain. Below, we present key drivers of FGM in Egypt and the risk factors that make some girls and women more vulnerable to the practice.
FGM as a rite of passage
FGM is traditionally seen as a rite of passage for marriageability. More than 50% of girls are cut between 9 and 12 years – an age which coincides with puberty, completion of primary school – and for some girls – marriage.8 Younger ages of cutting have been associated with child marriage in Egypt.12,13 Girls who continue their education are more likely to marry at an older age.
Parents’ experiences of FGM
FGM is perpetuated by parents’ experiences, attitudes and decisions. Parents with less education, lower income or who reside in rural areas are more likely to support continuing the practice of FGM.14,15 In rural areas, where stricter patriarchal structures predominate, FGM is more prevalent (90%) compared to urban areas (79%).8 Women’s experiences of FGM and age at marriage influences decision-making about FGM in their daughters, with girls more likely to undergo FGM if their mothers did. Mothers typically hold primary responsibility for decision-making around FGM, but grandmothers, aunts, and fathers also play a role. The medicalisation of FGM has likely increased fathers’ involvement due to the financial cost and the cultural expectation that women and children often need men’s permission to attend health clinics.16,17
Purity and family honour
The cultural and religious expectations of feminine purity and control over women’s sexuality are closely tied to the practice of FGM. It is performed under the notion that FGM is essential to reduce girls’ sexual appetites. According to a nationwide survey in 2015, 49% of men and 43% of women believed that FGM prevented adultery by women after marriage.18 Similar percentages of men and women (50% and 46% respectively) also believed that FGM was required by Islam.18 Performing FGM therefore signals to others that parents are ensuring a girl’s proper upbringing, while girls and women who submit to it demonstrate that they are concerned with preserving family honour.14
The practice of FGM also sits within a wider set of patriarchal customary and legal marriage norms that emphasise family honour and control over women. These include a preference for people to marry within the community (endogamy); and the tradition of married couples living with or near the husband’s family.19,20 The transfer of dowry/bride wealth payments also brings economic benefits to marriage and there is some evidence that girls and women who have had FGM may receive larger dowries.21 Extended families therefore play a crucial role in preserving and evolving attitudes towards FGM and other cultural and gender norms within religious and legal structures.
Medicalisation of FGM
Egypt is leading the way in the medicalisation of FGM globally, with healthcare providers involved in perpetuating the practice. While the last 20 years have seen a shift away from the use of traditional practitioners (‘dayat’, or traditional birth attendants, who tend to be women), there has been a dramatic increase in FGM in health facilities.22 Medical providers have been involved in FGM practices for decades, particularly doctors (of both sexes). Between 1995 and 2021, the proportion of girls and young women aged 19 years and younger who underwent FGM by a medical provider rose from 55% to 83%, with 74% of cases in 2021 performed by doctors.
Medical provision of FGM is prevalent across all regions of Egypt. Girls from higher-income households and those with higher levels of education are more likely to undergo medicalised FGM.23 The mother’s social and economic status particularly influences the likelihood of her daughter being subjected to medicalised FGM, with higher rates found among mothers from wealthier households and those with at least primary education, compared to those with no education.24
Parents are turning to medical professionals to perform FGM, believing it reduces the risk of complications like haemorrhaging and infection. Since medicalised FGM is illegal, it is usually carried out in secret within private clinics, in homes or hospitals. According to research conducted in 2019, the cost of FGM ranged from 250 to 1,500 Egyptian pounds (USD 14-85), though this is likely higher now when accounting for inflation in Egypt. Costs depend on factors such as the type of anaesthesia used, hospital fees, and the procedure recommended or selected, which is determined in part through a practitioner’s examination of the girl’s anatomy for cosmetic reasons.22
Reasons behind FGM medicalisation, as opposed to outright rejection of the practice, are multifaceted. Initially, advocacy and policy efforts focused on highlighting the immediate health risks associated with FGM by traditional midwives, rather than framing FGM as a human rights or legal issue. Accordingly, parents now choose medical practitioners to perform FGM, believing that they are better able to prevent health risks associated with the practice.16 This means the underlying cultural and societal factors driving the practice largely remain unaddressed.
Attitudes among medical providers also need to shift. Refaat (2009)25 found that while 29% of doctors who performed FGM reportedly did so to reduce the harm of parents sending their daughters to traditional midwives; 51% did so out of a belief that FGM was beneficial to women and girls – particularly when an ‘enlarged’ clitoris was present. The rest (19%) did so for financial reasons. In another study, some doctors admitted that financial incentives were their primary motivator, even though they were aware of the associated risks and illegality. They expressed that medicalised FGM is promoted by healthcare providers and that they can easily convince people to undergo it.22 Social pressures may also drive some providers to perform FGM; for example, if they fear a loss of respect and trust from rural communities for refusing to cut girls.22 Some doctors also tolerate the practice even if they do not believe in it and are willing to refer parents to other health providers.
Interventions against FGM in Egypt
Interventions to discourage FGM in Egypt have evolved from focusing mainly on health risks promoting medicalisation to a broader rights-based framework focused on gender equity. The need to protect people experiencing forced migration in Egypt from FGM has so far been addressed mainly in an ad hoc way.
Initial efforts began in the 1920s with the Egyptian Physicians Association called for a ban on FGM due to its health risks. By 1959, the Ministry of Public Health prohibited the most severe form of FGM (Type 3) but allowed partial clitoridectomy under medical supervision. The 1990s marked a pivotal shift, with the 1994 International Conference on Population and Development broadening the discussion to human and women’s rights. The practice was banned in hospitals in 1996, though a loophole for ‘medically necessary FGM’ (for enlarged clitorises) persisted until 2007.26 Public outcry over FGM-related deaths led to the adoption of a law banning the practice in 2008 for all children in Egypt, irrespective of their nationality. The same year witnessed the launch of the UNFPA-UNICEF joint programme for the elimination of FGM in Egypt, which emphasised women’s and girls’ rights. Actions have focused on policy and legal reform; strengthening appropriate and quality services, and information systems; and increasing community awareness from legal, medical and religious perspectives.
Efforts by the National Council for Women and the National Council for Childhood and Motherhood have also helped ensure FGM is a national priority; they developed a national FGM abandonment strategy (2016-2020) and action plan (2022) and included FGM in the National Strategy for the Empowerment of Egyptian Women (2030). Under the auspices of Egypt’s First Lady, the National Girls’ Empowerment Initiative (which focuses on empowering girls and challenging traditional gender roles) also aims to reduce the pressure on families to continue the practice of FGM. The initiative incorporates the Dawwie programme (‘sound with an echo’ in English) which seeks to create safe supportive spaces for girls to express themselves; to share their stories to inspire others; and to link them with youth centres and clinics.27 It also incorporates the Noura mentorship programme, which links young adolescent girls (aged 10-14) with older girls and women (aged 18-20) in rural villages. This forms part of the President’s human development initiative, Haya Karima (‘decent life’ in English).28 While these initiatives aim to engage school-age girls, FGM activities are not yet integrated into the Egyptian school curriculum.
Addressing deep-rooted social norms surrounding FGM is a key feature of these and other programmes. National door-knocking campaigns are used to provide advice on FGM through home visits. Mass media campaigns and social media efforts have involved celebrities, medical professionals, and religious leaders to influence public opinion. The youth organisation, Y-Peer has used interactive street theatre and peer-to-peer initiatives to engage youth and communities in dialogue about FGM. A critical part of these efforts has been distancing FGM from religious beliefs. Partnerships between the UN Joint Programme; the prestigious university of Islamic learning, Al-Azhar University; and the Coptic Church, have led to public declarations denouncing FGM from both the Grand Imam and the Pope.
Efforts to protect girls at risk and support survivors are also central to the interventions. Child protection systems, strengthened health services, and social worker training are key components of prevention and care services. These services provide medical, psychological and legal support to survivors and aim to prevent FGM through parental counselling and community outreach. Additionally, Egypt’s Child Helpline serves as a reporting mechanism for potential FGM cases, ensuring that violations are addressed through appropriate channels.
In 2021, the penal code was amended and stipulates imprisonment for up to 20 years for doctors and other medical personnel who are convicted of practicing FGM. It also stipulates the closure of medical facilities where FGM is performed, if the owner is aware that FGM is being performed there. Additionally, the law introduces penalties for those who advocate for or promote FGM, even if the promotion does not lead to the procedure being carried out.
The FGM experiences of Sudanese refugees living in Egypt were part of civil society advocacy that brought about national-level changes in the late 1990s.29 Additionally, interventions addressing FGM among displaced populations in Egypt have been part of broader humanitarian response efforts for several years. However, these efforts are still characterised by their ad-hoc nature. Further, while more activities engage displaced populations from African countries where FGM is highly prevalent, engagement materials and approaches are not tailored to displaced populations’ diverse cultural contexts.30 Interventions for displaced populations largely mirror the structure of national FGM interventions, particularly focusing on prevention activities such as awareness-raising campaigns.
Protection services, such as access to medical care and referrals for girls at risk of FGM and FGM survivors, is not always available to all displaced groups. Asylum-seekers and undocumented migrants, for instance, can face exclusion from these services depending on whether the provider is a public institution or an NGO. The geographic and linguistic availability of services also varies, creating gaps in protection and care for the most vulnerable populations – especially those without official refugee status.
Context of FGM in Sudan
Like Egypt, Sudan also has one of the highest prevalences of FGM globally, reaching 87% among women aged (15-49) and 31% among girls (0-14).31 As shown in Figure 2, FGM is more prevalent in northern states than southern ones, with the exception of East Darfur. Sudan is ethnically diverse and different groups have different practices and traditions associated with FGM. For example, central and west Darfur have lower state-wide rates of FGM because the Fur, Hawsa and Umbarraro ethnic groups who live there do not traditionally practice FGM. Despite the high prevalence of FGM, there have been notable changes in the practice across the country. One significant shift is from the predominance of the infibulation-type cut (Type 3) to greater use of the less severe Type 1. This change is likely to have been influenced by growing medical advocacy highlighting the severe health risks associated with Type 3.32
As in Egypt, there has been a trend towards the medicalisation of FGM driven by concerns about health risks associated with methods used by traditional midwives and circumcisers. The proportion of women aged 15-49 who underwent FGM performed by medical professionals increased from 55% in the period 1966-1979, to 76% in the period 2000-2014.33 There are large differences by state, with 94% of women in Khartoum state (incorporating the capital) reporting undergoing FGM by a medical professional, compared to 43% in neighbouring rural Gedaref state in 2014.34 Unlike in Egypt, nurses and midwives (rather than doctors) tend to deliver FGM in Sudan and most of these practitioners are women.
Figure 2. Heat map showing FGM prevalence among women (15-49) by state in Sudan
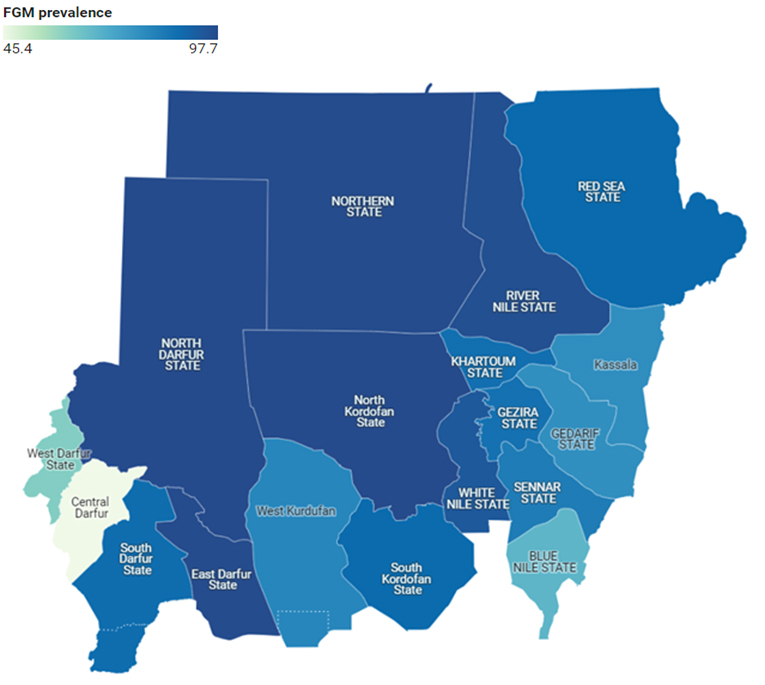
Source: Author’s own. Created using Datawrapper. Based on UNICEF MICS (2014)31 data.
Drivers and risk factors for FGM in Sudan
The age at which cutting occurs is generally younger in Sudan than Egypt. In Sudan, over 60% of girls in 2014 (the most recent year for which data is available) had undergone FGM between the ages of 5 and 9, with a mean age of 5.7 years.31 The age of cutting varies culturally and ethnically. For example, among the Meloha in Gedaref state, FGM is traditionally practiced soon after birth by the same midwife who delivered the baby.34 Nationwide, there has been a modest trend toward a higher age of cutting over the prior three decades; the proportion of girls cut at age 10 or older increased from 10% during 1980-1989 to 23% during 2000-2014.33 The risk of undergoing FGM was greater for girls (aged 0-14) from rural households than their urban counterparts. Mothers with higher levels of education and those who married at a later age were less likely to subject their daughters to FGM compared to mothers with no education or those who married at a younger age.33
Communally, the motivations for practicing FGM in Sudan are similar to those in Egypt and neighbouring countries. These motivations include religious beliefs; cultural beliefs (enhancing girls’ marriageability); and safeguarding their virginity, with FGM perceived to improve cleanliness, femininity and beauty.35Gender norms often reinforce the belief that FGM controls female sexuality, framing women’s bodies as objects for male sexual pleasure.
Re-infibulation (known as ‘adal’), the process of re-sewing the genitals following childbirth, is also common among Sudanese women. Although it is not as prevalent as infibulation and has decreased over time, in 2014 re-infibulation was performed on around one in four (23.9%) of ever-married women aged 15-49 who had given birth.31 In a surveillance study of sites in Khartoum and Gedarif, around one-third of women underwent re-infibulation after birth.36
Re-infibulation is also sometimes performed for elderly women as a ‘purification’ rite before death.36 At younger ages, FGM may sometimes be practiced to treat illness, for example in female toddlers who appear sickly.34 Some communities believe FGM protects against infertility and stillbirth.37
FGM can be a taboo. Many men say they do not know if their female relatives have undergone the practice.38 Qualitative research in 2019 suggested that when women and men claim to have stopped practicing FGM, they are mainly referring to infibulation (Type 3) and are still likely to practice Type 1.34 Nonetheless, there seems to be a shift in social attitudes away from FGM. Over half of women aged 15-49 (52.8%) now report advocating for its abandonment, particularly in urban areas and in states with anti-FGM interventions.33 Sudanese activists also describe vibrant public debate on social media platforms, with young people demonstrating their rejection of FGM alongside a commitment to stay true to Sudanese values and traditions in other ways.37
Interventions against FGM in Sudan
Efforts to ban or eliminate FGM in Sudan can be traced to at least the 1940s but have not resulted in large-scale behaviour change until very recently.37 Sudan adopted a 10-year multi-sectoral strategy to address FGM in 2008, starting with social and legal interventions in several southern states including South Kordofan, Gedaref, Blue Nile, Kassala, River Nile and South Darfur.
A nationwide campaign designed to create positive cultural associations with abandoning FGM worked with activists to identify and introduce a new term for girls remaining uncut: ‘saleema’.39 Previously, while circumcised girls were commonly described as clean and pure, uncut girls were often described by the derogatory term, ‘ghalfa’ (suggesting disgrace, degradation and inappropriate behaviour). The campaign adopted the Arabic word, ‘saleema’ (meaning ‘whole, healthy in body and mind, unharmed, pristine and perfect in God-given condition’).40 This term was used to brand a variety of anti-FGM activities involving community leaders, religious scholars and clerics who stressed the legitimacy and permissibility of leaving the girl saleema (intact and perfectly healthy) from the religious point of view. The campaign measured a significant decrease in pro-FGM social norms among people exposed to the campaign in 2016-2017.41
Between 2016 and 2018, health sector interventions were added to address medicalisation. A third of practising community midwives (healthcare professionals with one year of nurse training) received training on managing FGM complications and signed a commitment to end FGM. Facility-based midwives and other practitioners, including nursing and medical students, were also reached through interventions such as developing training curricula and professional codes of conduct.36 Research from intervention areas suggests that professional midwives’ refusal to practice FGM has led to an increased understanding of the illegality of FGM, particularly Type 3. However, some families also reported turning away from these midwives not just for FGM but also for other midwifery needs, preferring traditional midwives (‘dayat al-jabal’) for FGM and female relatives to deliver babies for women who have been cut.34
Legal changes to prevent FGM happened later in Sudan than in Egypt, coinciding with the brief period of joint military-civilian rule between 2019 and 2023 that saw progress on many women’s rights issues in Sudan.38 Civil society actors successfully campaigned to criminalise the infibulation form of FGM in some states before this. However, federal-level attempts to criminalise all forms had always been blocked, including through a fatwa of the Islamic Jurisprudence Council in 2010 which saw Type 1 FGM reinforced as Sunnah.37 In July 2020, a national law against FGM was adopted criminalising all forms of FGM, which covered the whole of Sudan for the first time. Medical providers and traditional practitioners who perform FGM can now be fined and imprisoned for three years.
It is unclear how the dramatic increase in fighting since 2023 may affect anti-FGM work and provision of FGM by nurses and midwives. Despite disruptions to nationwide anti-FGM programming led by UNFPA and UNICEF during the COVID-19 pandemic, many grassroots organisations and civil society networks were able to develop simple but effective activities. These paved the way for continued local level action during the crisis. For instance, local protection networks in Khartoum, East Darfur and elsewhere visited the parents of newborn girls to discuss FGM abandonment over tea.42,43 Further, the youth network, Y-Peer, helped establish school clubs to discuss FGM with children, parents and other community members.42
Healthcare infrastructure has been severely weakened by attacks on health facilities and the abandonment of hospitals by staff, especially in the capital, Khartoum. Combined with a dramatic increase in sexual violence, reduced access to reproductive health services and the anti-FGM interventions of the last few years, midwives in Sudan may now be less inclined or able to offer FGM services.44 Nevertheless, financial incentives have always been an important reason for midwives to offer FGM services in the pre-crisis context of high unemployment for health workers and low government salaries.36 These financial pressures are magnified in the current context of acute conflict and displacement.
Displacement in Egypt
Egypt hosts forcibly displaced populations from 62 countries.45 Displaced populations from Sudan, which shares a border with Egypt, are the largest group. Syrians form the second largest displaced group, followed by South Sudan, Eritrea, Ethiopia, Yemen, Iraq and Somalia. The two nations (Egypt and Sudan) were one country until 1956, when Sudan voted for self-determination at the end of Anglo-Egyptian rule. As such, there is a long history of Sudanese people migrating to Egypt for safety, economic, educational, social and other opportunities.
Egypt has seen the largest influx of asylum-seekers in the region since the escalation of armed conflict in Sudan. Around 61,000 Sudanese people were registered with UNHCR before April 2023, but the conflict is estimated to have prompted around 1.2 million to flee to Egypt.46 Less than half are registered (around 504,000 as of 2 Oct 2024).46 Many families were separated, and many women took their children to Egypt without their husbands. Children under 18 form around 40% of the displaced population.45 Around 84% of recent arrivals report coming from Khartoum, reflecting the severe impact of the conflict on families and children in the capital.47
Figure 3. Heat map showing the concentration of refugees and asylum-seekers across Egypt
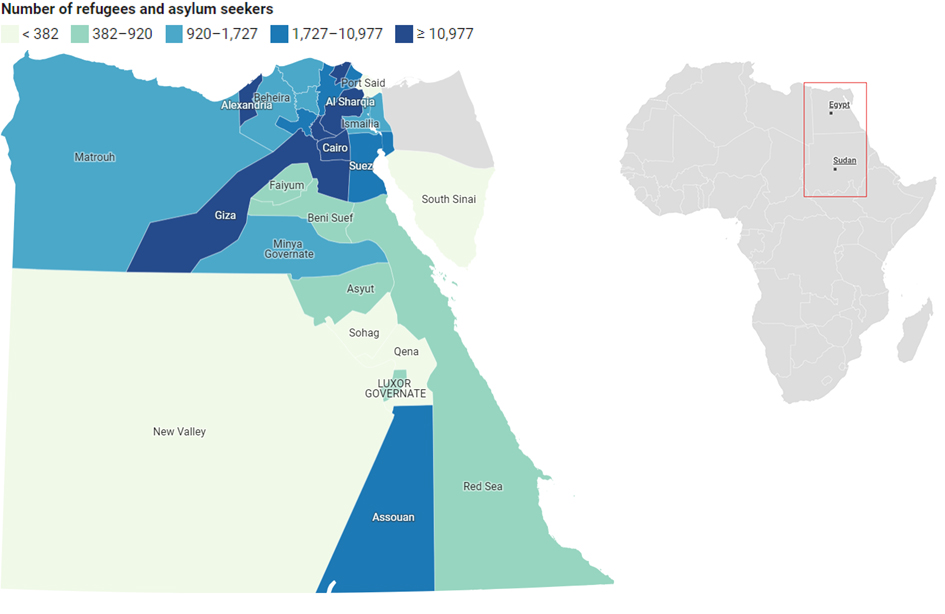
Source: Author’s own. Created using Datawrapper. Based on data for officially registered refugees and asylum-seekers publicly available from UNHCR.48
Notes: Heat map shows the concentration of refugees and asylum-seekers across Egypt (left); continent inset shows the location of Egypt and Sudan (right).
As shown in Figure 3, refugees and asylum-seekers in Egypt are primarily located in the north-east of the country (‘lower Egypt’) within urban neighbourhoods of Greater Cairo, Alexandria, Damietta and other cities. Many people who have newly arrived from Sudan have also settled around Aswan in southern (‘upper’) Egypt, close to the border with Sudan. Here, UNHCR offers temporary accommodation for people in transit to other parts of the country and supports them with protection and other services. However, to register as an asylum-seeker with UNHCR and obtain a residency permit from the Egyptian government, Sudanese people must travel to UNHCR offices in Greater Cairo.
Entry restrictions for Sudanese have been tightened since June 2023. There is currently a large backlog of visa applications at Egyptian representative offices in Sudan and for asylum-seeking and refugee status applications at UNHCR offices in Egypt. The complexity of the registration and visa process means that many Sudanese people now cross the border and complete their northwards journey with the assistance of smugglers.49 Smugglers charge around 500 USD per person, and migrants are subjected to exploitation, violence and abuse along the journey, including during interactions with local authorities.49,50 Children are especially at risk of exploitation, human trafficking, sexual violence and death. Moreover, those who come to Egypt through smuggling face the risk of being arrested, detained and deported.49
Reasons for people to remain in or return to Aswan include not having resources to continue travelling or wanting to stay close to the border for return or circular migration. A desire to remain amongst a Sudanese community with shared experiences of trauma and displacement might also be important. This is in the context of discrimination and economic exploitation historically faced by Sudanese people in lower Egypt, which continues today in a context of economic stress and rising inflation.
Living conditions are very poor for most Sudanese displaced populations. Many people live within informal settlements, for example in unfinished tower blocks on the outskirts of Cairo. Many lack stable sources of income, with limited livelihood opportunities. Access to most public services in Egypt, including school, requires people to be registered as refugees. An important initiative of Sudanese civil society in Egypt was the establishment of community schools and nurseries so women could have time to work.51 However, government immigration crack-downs since July 2024 have successfully closed down many Sudanese schools, restaurants and businesses for being unlicensed, or not having permits.50 Many Sudanese now report being afraid to leave their house.49,50
FGM and forced displacement
Little is known about how conflict and migration dynamics affect FGM practices in low- and middle-income country settings hosting forcibly displaced populations, including how social norms from the country of origin and host community interact.50,52 Some key drivers are discussed below.
Early marriage and FGM as ‘protective’ against sexual violence. In several contexts of forced displacement across Africa and the Middle East and across rural and urban settings,53,54 early marriage is felt to be protective for displaced girls who are seen to face more sexual violence from strangers than married girls and women. Early marriage to avoid sexual violence or bad behaviour because of ‘idleness’ in displacement settings helps preserve family honour.53. In Egypt, protection concerns and other displacement-specific challenges such as disruptions to girls’ education have been found to exacerbate girls’ vulnerability to child marriage for some displaced families from Syria. For others, displacement to urban areas seemed to erode pre-war norms and marriages were delayed.55
The practice of FGM is also associated with parents trying to control their daughters in the displacement environment and efforts to prevent them from being the victims of sexual violence, including rape.52 For Somali refugee families in Ethiopia, the fear of sexual violence has previously been identified as a factor that can drive families to subject their daughters to FGM.56 Similar beliefs may be held among Sudanese displaced communities in Egypt. One humanitarian practitioner interviewed for this brief explained there is a common mindset that: ‘Girls might be subjected to rape and assaults here but if she is subjected to FGM [infibulation], it will be hard to break her hymen so she will still be a virgin’. This is a dangerous perception, however. Young girls who have been subjected to FGM and then rape can face severe physical trauma and psychosocial complications; early pregnancies in these circumstances can also be very dangerous.57
The dark nexus of armed conflict and FGM. FGM is sometimes used as a method of torture and a means of exerting control over communities, particularly targeting women and girls.58 Attacks on women may specifically target them as the ‘carriers’ of future generations of the ‘enemy’, leading to horrific acts such as the mutilation of their genitalia or the destruction of foetuses. Acts of this brutal violence have been documented in Sudan and various recent conflicts in Africa, where women’s genitalia have been mutilated after rape or displayed as trophies of war. This underscores the urgent need for comprehensive interventions that address both GBV and FGM within the context of armed conflict and women’s rights.59
Economic pressures. In Ethiopia, the lack of income for refugee women circumcisers from Somalia contributed to their need to continue providing FGM services, and the desire of families to support these trusted women. 56 Being out of school because of COVID-19 lockdowns and economic pressures on parents was associated with an increase in FGM among girls from displaced populations in Uganda and Nigeria.7 Girls who are orphaned or separated from family by an emergency may be more likely to have to enter into forced early marriages and have FGM forced on them by others.35 FGM is also associated with preparing girls for commercial sex work in some displacement settings.35 Given the association between FGM, marriage and transfer of dowry, humanitarian practitioners in Egypt consulted for this brief also believe that Sudanese displaced communities see FGM and early marriage as a solution to the intense financial pressures displaced families face.
FGM as a familiar tradition. Displacement and associated processes of marginalisation intensifies the need for social belonging and familiar traditions. FGM is sometimes seen as a cultural identifier tied to marriage, virginity and honour, which can be reassuring to people displaced from their homes.7 Humanitarian practitioners in Egypt interviewed for this brief have discussed that an important reason Sudanese people are opting for FGM is so girls can continue to undergo an important rite of passage linked to girls’ marriageability. Male relatives can be important change agents within Sudanese society, leveraging their social power to challenge traditional norms.16 However, many displaced women making decisions for their daughters in Egypt are separated from their husbands. Research conducted in Khartoum emphasises that grandmothers, aunts and female in-laws can be influential in pressuring mothers who would prefer not to have their girls cut and intervene after mothers are deceased:
‘Pharaonic circumcision (Type 3 FGM) is very deep in our culture and we will not give it up. We have inherited it from our grandmothers. We will ensure it is done if a mother died, then an aunt or the grandmother will get it done.’
(25-30 year old respondent, Khartoum)34
Host community pressure. Undergoing FGM can also be used to establish or uphold social status in a new society where the practice is common. There are examples from Mali and Nigeria of internally displaced populations practicing FGM only after displacement.7,60 In Sudan, internally displaced communities in Blue Nile state and South Sudanese women in Khartoum have been observed to adopt FGM as a means of conforming with their host community’s social norms.42,61 Similarly, media reports from Egypt suggest that Syrian displaced populations have begun practicing FGM on their daughters to adapt to the local culture, likely influenced by economic pressure and concerns about girls’ marriageability.62 Humanitarian practitioners consulted for this brief additionally suggested that Syrian parents may have decided mistakenly, believing FGM to be a religious requirement in Egypt.
Insufficient civil society action and humanitarian response. Crises disrupt government and civil society programmes against FGM. In conflict-affected and displacement settings, the prevention of and response to FGM is often not prioritised in humanitarian settings due to lack of funding and political will.30 Groups practicing FGM from Blue Nile state that were displaced to South Sudan were observed to continue FGM in all refugee camps, apart from one where FGM awareness-raising campaigns were operating.63
Considerations for FGM cross-cultural transfer
In both Sudan and Egypt, FGM is a highly prevalent practice which is deeply embedded as a social norm. The shift in the cutting age in Sudan to higher age groups, towards Type 1 and 2 and medicalisation suggests a possible convergence in the FGM practice over the years between Sudan and Egypt. Nevertheless, there are regional differences and other dynamics that informants consulted for this brief recommend should be considered in the potential for cross-cultural transfer of FGM attitudes and practices,52 each of which might also be influenced by the length of displaced people’s stay:
- More Sudanese people may be influenced to transition to or maintain a preference for Type 1 and Type 2, especially in areas of lower Egypt where these types are prevalent.
- Especially for families from Khartoum who have a preference for medicalised FGM, it may be hindered or delayed if families cannot identify Egyptian practitioners working clandestinely; are afraid to use illegal services; or if they prefer not to take their girls to a male doctor.34
- Based on interviews with humanitarian practitioners in Egypt, some displaced girls are reportedly returning on short visits with their families to Sudan to undergo FGM in their ‘home’ communities. If the security situation improves over time, this movement may increase, raising concerns about the continuation of FGM practices across borders.
- Infibulation and re-infibulation currently take place in Egypt at lower levels compared to Sudan, including southern governorates like Aswan. However, more Egyptians could be influenced to adopt these practices through interactions with Sudanese communities, especially if there are practitioners in the host or displaced populations that are willing to conduct Type 3 FGM in response to demand.
Opportunities for intervention
Activities aimed at addressing FGM in forcibly displaced populations in Egypt are part of broader emergency response operations led by UNHCR, coordinated through monthly inter-agency meetings involving government, international, national and local organisations as well as consultations with communities. Activities on FGM are integrated into multi-sectoral humanitarian protection responses to address GBV, alongside provision of food, shelter, education, health, livelihood and other services. Asylum-seekers may not always be eligible or able to access these humanitarian initiatives. Evidence from other emergency settings suggests that FGM situational analyses are helpful when jointly conducted by development, humanitarian and local actors (including displaced populations). This helps to support the selection of shared outcomes for long-term programming initiatives and tracking.7
Partnering with Sudanese actors and initiatives
Partner with existing groups and activists with an interest in FGM. Local activists and grassroots organisations are often best placed to know and understand the challenges and social norms still driving FGM and are trusted by communities.37 Given that FGM practices in displacement can be driven by a desire to maintain a cultural identity, national and international initiatives seeking to address FGM in Egypt should consider the connections they can foster with Sudanese civil society in Egypt, Sudan and the Sudanese diaspora.
Key contributors to the Sudanese anti-FGM movement include the National Council for Child Welfare, non-governmental and civil society organisations, healthcare professional organisations, universities and media groups. Most state-level councils and steering committees formed before the civil uprising in 2018 have folded. Still, many of the individuals who have participated in these groups as well as grassroots initiatives to connect women’s groups with religious and community leaders, midwives, youth and children’s groups are likely to remain personally committed to change.37 Sudanese midwives within the displaced population, some of whom may have recently made pledges to abandon FGM, might be particularly influential and could offer personal testimonies about the ill effects of cutting.
Partner with new forms of civil society action. As with displaced populations in Egypt, large populations of Sudan have also been internally displaced and are establishing new social structures in displacement. Community-driven, and often women-led, mutual aid efforts that have built on the peaceful uprisings against military rule could be used to mainstream FGM-related interventions as they respond to emerging humanitarian needs. In Egypt, community-led schools and nurseries established by and for Sudanese displaced people could be important collaborating actors for developing child-centred FGM programming for migrant populations who may be excluded from Egyptian initiatives targeting school-aged children.
Be sensitive to immigration risks. When considering how to integrate displaced communities into national and civil society-run FGM initiatives, programmes should be mindful of Sudanese people’s fears of being identified by authorities for irregular immigration. Particularly in door-knocking campaigns, every effort should be made to collaborate with Sudanese community organisations and incorporate their volunteers or staff to alleviate fears and enable community entry.
Involve displaced populations in research on how FGM is changing. Specific research is also needed on how FGM practices and attitudes are evolving in different Sudanese and other displaced populations in Egypt to help responding agencies assess needs and design appropriate protection strategies. Research on FGM could consider adopting co-production principles with displaced people as co-researchers to contribute to women’s and displaced populations’ empowerment and support future uptake of the findings.
Information-sharing and dialogue on FGM
Discuss FGM holistically. Responding agencies try to reach diverse displaced communities in Egypt, whether or not they come from cultures with existing FGM practices. Information-sharing initiatives typically take a holistic approach involving collaborations with local religious leaders and doctors to discuss legal, religious and medical aspects. This approach has arisen because of agency experiences of the limitations in discussing the harms of FGM to health more narrowly:
‘One issue that we confront is that a lot of women are already cut and do not feel or experience any harm from FGM, so when we lecture about the harm of FGM and say it causes such and such, they think “well, that didn’t happen to me, so you are probably lying”. This is why exaggeration in awareness sessions is a problem.’
(UNFPA, 2021)30
The psychosocial harms of FGM may be particularly underappreciated. When FGM is not recognised as a harmful practice, individuals eligible for FGM support services in Egypt may not receive the assistance they need.
Tailor FGM information to different groups’ needs and contexts. Sessions also typically try to incorporate information relevant to people with different nationalities, as described by one humanitarian actor consulted for this brief:
‘Drivers for FGM might be the same among different nationalities with some differences […] for example Sudanese are mostly motivated by girls’ marriageability while Egyptians might be more motivated by the religious aspect.’
(Sudanese community health volunteer, Egypt)
The large number of displaced populations from diverse countries living in Cairo means that responding agencies have historically had difficulty differentiating community engagement materials for different communities.30 On the one hand, anti-FGM interventions can transcend nationality and ethnicity by appealing to the universality of women’s and girls’ rights.44 Having a core set of information about the risks of FGM in the Egyptian context is also helpful since many displaced groups are exposed to the same drivers and risks within Egyptian society. On the other hand, some displaced communities have much more deeply entrenched FGM practices. This demonstrates the need for contextualised approaches that are carefully tailored to community needs. Sudanese displaced communities themselves will also have members with very different levels of education and knowledge about FGM and require tailored information.
Use social media effectively. Media and social media, including the use of videos to reach children, can be highly influential in shifting attitudes about FGM. These are reported to have been historically underused in humanitarian response activities in Egypt,30 but many NGO and national initiatives, such as Dawwie, have an online presence. These initiatives could change this if they could be extended to displaced communities. 27
Involve men and boys. Humanitarian practitioners consulted for this brief noted that there is a lack of engagement of men and boys as central actors in FGM prevention strategies where some organisations focus on women and girls and others include them only in awareness-raising sessions. Men’s involvement is essential in breaking the cycle of FGM due to their influential positions within families and communities and will alleviate social pressure on women to uphold harmful traditions. Interventions should focus on engaging men and boys as active volunteers, service providers, and community leaders, empowering them to take on meaningful roles in fostering gender equality and preventing FGM.
Discuss ‘culture’ sensitively. A common challenge faced by anti-FGM campaigns globally is to frame messages positively and avoid creating stories about ‘victims’ who suffer because of their ‘backward and barbaric’ culture. Criticising an entire culture ignores that culture itself is diverse and fluid. It also risks alienating people who can be change agents to trigger lasting and widespread rejection of FGM. Sudanese people in Egypt often report feeling discriminated against64 and populations within Sudan have been the object of international funding and attention to eradicate FGM for decades.37 Egyptian and global organisations seeking to talk about FGM with Sudanese displaced populations should therefore take care to adopt culturally sensitive approaches. They could invest in community engagement, capacity building, and partnerships to effectively address FGM and support women and girls affected by it.
Be sensitive to FGM survivors in messaging and the ways services are organised. Community engagement approaches should be sensitive in the ways they discuss FGM abandonment and harms and anticipate the effects on survivors. Informants consulted for this brief emphasised that many young girls experience depression and trauma upon realising the implications of FGM, leading to difficulties in accepting their bodies and feeling ashamed. Affected women should be involved in crafting and reviewing community engagement messages to avoid unintentionally creating harms. Strict confidentiality protocols, including discreet access to services, are also essential to prevent stigma and shame, enabling women to seek help without fear of exposure.
Use materials already tailored to Sudanese peoples’ needs. Organisations seeking to promote FGM abandonment among Sudanese displaced populations could consider drawing on materials and approaches developed for Egyptian populations as well as those previously developed for Sudan. The Saleema Initiative39, for example, was developed through long-term collaborations between the Sudan government, UN institutions, Sudanese academics and civil society. These ideas may already be familiar to many Sudanese populations from different areas of the country.
As of late 2022, the remaining issues that UNICEF recommended organisations take up to address FGM in Sudanese populations included working with religious leaders to develop new narratives and arguments to support collective abandonment of FGM. It emphasised shifting advocacy messages away from hazards and negative implications of FGM and toward the health, hygiene and other benefits of abandoning the practice.65 New messages can be co-developed with displaced parents, women’s groups and leaders to ensure they reflect realities and concerns in the new displacement environment. The approaches developed by Y-Peer in Sudan to engage children and their parents through school clubs could also be effective in Egypt.
Strengthen capacities and protect volunteers. In Egypt, informants consulted for this brief felt that community outreach activities undertaken by displaced volunteers were a successful approach for engaging with displaced communities and also identifying girls at risk of FGM:
‘One of the most important interventions are the community outreach ones, we mainly apply it through trained volunteers from the same nationality of the refugee community and that helps understand and customise the awareness based on the community needs.’
(Humanitarian project manager, Egypt)
Programmes using volunteers to discuss FGM should be sensitive to the complexity of displaced workers’ circumstances and relationships with other community members and support them in delivering their duties. In Kenya, refugee workers attempting to discuss FGM have faced opposition from their communities who view them as ‘un-Islamic’ and ‘going against culture’ as well as personal security challenges, highlighting the need to invest in support for displaced workers in humanitarian programmes.66 Programmes in Egypt should aim to strengthen the knowledge and capacities of displaced workers so that they can confidently and sensitively discuss the far-reaching impacts of FGM on girls’ and women’s lives and also work with volunteers to create supportive team dynamics to solve problems as they arise.
Case management, referrals and support for survivors
Recognise the multi-dimensional needs of survivors. Case management focuses on identifying survivors of violence and referring them to medical, legal, and/or psychosocial counselling services. In humanitarian responses, case management is used for all types of GBV, including FGM. However, in Egypt survivors of FGM tend not to voluntarily report and only come to the attention of programmes when they need medical support.30 It is therefore important to integrate questions that systematically enquire about FGM in routine screenings for violence. Linking to or involving Sudanese groups providing psychosocial support in Egypt would also be beneficial.
Build the capacity of midwives to support women with Type 3 FGM. In countries where FGM is uncommon, health providers are often unaware of the challenges confronting cut women during delivery and their higher risks for infections and complications.7 Similar challenges could affect Sudanese women with Type 3 FGM being assisted by providers in Egypt who are more familiar with delivering babies from women affected by Type 1 and Type 2. Collaborating with Sudanese obstetricians and midwives in Egypt can enhance reciprocal capacity-building.
Share information about legal risks of FGM with displaced populations. In displacement settings, migrant populations and migrant health workers are often more vulnerable to incarceration, deportation and fines. They are also at risk of exploitation due to wanting to avoid attention from police and authorities.67 Discussions about using illegal FGM services and channels to report incidents of FGM should address risks for families and FGM providers coming to the attention of authorities. Displaced communities, including displaced midwives, need to know the legal rules surrounding FGM in Egypt and organisations serving displaced populations can support this kind of information-sharing.
Empower survivors. Humanitarian practitioners consulted for this brief highlighted a lack of economic empowerment and livelihood activities that address the unique needs of forcibly displaced populations who are often systematically excluded from the labour market in Egypt. Only a few humanitarian organisations integrate vocational training with their FGM and GBV interventions. Women’s economic empowerment is an important factor influencing FGM practice, where economic resources could provide women with the power to oppose FGM and harmful practices that could affect their daughters negatively.68–70 Training programmes should be designed and delivered in consultation with displaced women to ensure relevant skills are taught and to enhance participation and empowerment. Art and sport therapy were also cited as beneficial for FGM survivors (including interactive theatre, psychodrama, Zumba and dancing classes, etc), helping displaced populations build connections with their community and spread anti-FGM awareness.
References
- UNICEF. (2024, March 7). Female Genital Mutilation: A global concern – 2024 update. https://reliefweb.int/report/world/female-genital-mutilation-global-concern-2024-update
- WHO. (2024, February 5). Female genital mutilation. https://www.who.int/news-room/fact-sheets/detail/female-genital-mutilation
- O’Neill, S., & Pallitto, C. (2021). The Consequences of Female Genital Mutilation on Psycho-Social Well-Being: A Systematic Review of Qualitative Research. Qualitative Health Research, 31(9), 1738. https://doi.org/10.1177/10497323211001862
- WHO. (n.d.). Types of female genital mutilation. https://www.who.int/teams/sexual-and-reproductive-health-and-research-(srh)/areas-of-work/female-genital-mutilation/types-of-female-genital-mutilation
- Ghanem, N. (2023). National Policies to End Female Genital Mutilation/Cutting in Egypt: An Analytical Review [Master’s Thesis, the American University in Cairo]. https://fount.aucegypt.edu/etds/2043
- Chatterjee, D. (2018, July 21). Tracing the Origins of Female Genital Cutting: How It All started. SAHIYO. https://sahiyo.com/2018/07/21/tracing-the-origins-of-female-genital-cutting-how-it-all-started/
- Elnakib, S., & Metzler, J. (2022). A scoping review of FGM in humanitarian settings: An overlooked phenomenon with lifelong consequences (p. 49).
- Central Agency for public mobilization and statistics (CAPMAS). (2022). Egypt Family Health Survey 2021. https://censusinfo.capmas.gov.eg/Metadata-en-v4.2/index.php/catalog/665
- Ministry of Health and Population [Egypt], El-Zanaty and Associates [Egypt], & ICF International. (2015). Egypt Demographic and Health Survey 2014. Ministry of Health and Population and ICF International. https://dhsprogram.com/publications/publication-FR302-DHS-Final-Reports.cfm
- El-Zanaty, F., & Way, A. A. (2001). Egypt Demographic and Health Survey 2000. Ministry of Health and Population [Egypt], National Population Council and ORC Macro.
- UNICEF, & UNFPA. (2019). Female Genital Mutilation (FGM) (UNICEF Egypt Data Snapshot – Issue 2).
- Elnakib, S., Elsallab, M., Wanis, M. A., Elshiwy, S., Krishnapalan, N. P., & Naja, N. A. (2022). Understanding the impacts of child marriage on the health and well-being of adolescent girls and young women residing in urban areas in Egypt. Reproductive Health, 19(1), 8. https://doi.org/10.1186/s12978-021-01315-4
- Karumbi, J., Gathara, D., & Muteshi-Strachan, J. (2017). Exploring the association between FGM/C and early/child marriage: A review of the evidence. Population Council. https://doi.org/10.31899/rh7.1019
- Van Rossem, R., Meekers, D., & Gage, A. J. (2016). Trends in attitudes towards female genital mutilation among ever-married Egyptian women, evidence from the Demographic and Health Surveys, 1995–2014: Paths of change. International Journal for Equity in Health, 15, 31. https://doi.org/10.1186/s12939-016-0324-x
- UNICEF, & UNFPA. (2021). Egypt (UNFPA-UNICEF Joint Programme on the Elimination of Female Genital Mutilation: Accelerating Change – 2021 Annual Report).
- Wahba, N., El Banhawi, H., & El Ayouti, A. (2020). Understanding female genital mutilation/cutting abandonment in Egypt. Population Council. https://doi.org/10.31899/rh11.1045
- El Feki, S., Heilman, B., & Barker, G. (2017). Understanding Masculinities: Results from the International Men and Gender Equality Survey (IMAGES) – Middle East and North Africa. UN Women and Promundo-US.
- Ministry of Health and Population [Egypt], El-Zanaty and Associates [Egypt], & ICF International. (2015). Egypt Health Issues Survey 2015. Ministry of Health and Population and ICF International.
- FCDO. (2023, April 18). Family law in Egypt. Foreign, Commonwealth & Development Office. https://www.gov.uk/government/publications/family-law-in-egypt/family-law-in-egypt
- Yount, K. M., Cheong, Y. F., Grose, R. G., & Hayford, S. R. (2020). Community gender systems and a daughter’s risk of female genital mutilation/cutting: Multilevel findings from Egypt. PLOS ONE, 15(3), e0229917. https://doi.org/10.1371/journal.pone.0229917
- Khalifa, S. (n.d.). Female Genital Cutting and Bride Price.
- El-Gibaly, O., Aziz, M., & Abou Hussein, S. (2019). Health care providers’ and mothers’ perceptions about the medicalization of female genital mutilation or cutting in Egypt: A cross-sectional qualitative study. BMC International Health and Human Rights, 19(1), 26. https://doi.org/10.1186/s12914-019-0202-x
- Aziz, M., Elgibaly, O., & Ibrahim, F. E. (2022). Effect of parental attitudes on the practice and medicalization of female genital mutilation: A secondary analysis of Egypt Health Issues Survey, 2015. BMC Women’s Health, 22(1), 259. https://doi.org/10.1186/s12905-022-01834-7
- Van Eekert, N., Leye, E., & Van de Velde, S. (2018). The Association Between Women’s Social Position and the Medicalization of Female Genital Cutting in Egypt. International Perspectives on Sexual and Reproductive Health, 44(3), 101–109. https://doi.org/10.1363/44e6618
- Refaat, A. (2009). Medicalization of female genital cutting in Egypt. Eastern Mediterranean Health Journal = La Revue De Sante De La Mediterranee Orientale = Al-Majallah Al-Sihhiyah Li-Sharq Al-Mutawassit, 15(6), 1379–1388.
- 28 Too Many. (2017). Country Profile: FGM in Egypt. https://www.refworld.org/docid/5a17ef454.html
- Dawwie. (n.d.). About Dawwie. Dawwie. https://dawwie.net/en/about-dawwie
- UNFPA. (n.d.). The Noura Framework. UNFPA Egypt. https://egypt.unfpa.org/en/Noura
- WHO. (1999). Female genital mutiliation programmes to date: What works and what doesn’t. World Health Organisation. https://iris.who.int/bitstream/handle/10665/65857/WHO_CHS_WMH_99.5.pdf
- Elnakib, S., UNFPA ASRO, & Metzler, J. (2021). Female Genital Mutilation in Humanitarian Settings in the Arab Region: Synthesis Report on Gaps and Priorities for Prevention and Response Programming (pp. 186–212). UNFPA and the Women’s Refugee Commission. https://www.tandfonline.com/doi/full/10.1080/07399332.2020.1789642
- Central Bureau of Statistics (CBS), & UNICEF Sudan. (2016). Multiple Indicator Cluster Survey 2014 of Sudan, Final Report. UNICEF and Central Bureau of Statistics (CBS).
- Bedri, N., Sherfi, H., Rudwan, G., Elhadi, S., & Elamin, W. (2018). Medicalisation of female genital mutilation/cutting in Sudan: Shift in types and providers. Reproductive Health. https://doi.org/10.31899/rh6.1023
- Thiam, M. (2016). Female Genital Mutilation/Cutting (FGM/C) and Child Marriage in Sudan—Are There Any Changes Taking Place? UNICEF, UNFPA, WHO.
- Bedri, N., Sherfi, H., Rudwan, G., Elhadi, S., Kabiru, C., & Amin, W. (2019). Shifts in FGM/C practice in Sudan: Communities’ perspectives and drivers. BMC Women’s Health, 19(1), 168. https://doi.org/10.1186/s12905-019-0863-6
- 28 Too Many. (2019). Country profile: FGM in Sudan, November 2019. https://www.fgmcri.org/media/uploads/Country%20Research%20and%20Resources/Sudan/sudan_country_profile_v1_(november_2019).pdf
- Ahmed, W., Puttkammer, N., Gloyd, S., Adam, A., Eltayeb, D., & Farquhar, C. (2022). Turning the tide on female genital mutilation in a high prevalence country: A programmatic data analysis for Sudan’s comprehensive health sector response, 2016–2018. BMJ Global Health, 7(10), e010020. https://doi.org/10.1136/bmjgh-2022-010020
- Bedri, N., & Bradley, T. (2017). Mapping the complexities and highlighting the dangers: The global drive to end FGM in the UK and Sudan. Progress in Development Studies, 17(1), 24–37. https://doi.org/10.1177/1464993416674299
- BBC. (2020, May 1). Sudan criminalises female genital mutilation (FGM). BBC. https://www.bbc.com/news/world-africa-52502489
- Saleema. (n.d.). Saleema—Initiative to stop FGM/C in Sudan. Saleema. https://www.saleema-sd.org/news.php
- UNICEF Sudan. (n.d.). Saleema Initiative. Retrieved 21 October 2024, from https://www.unicef.org/sudan/saleema-initiative
- Evans, W. D., Donahue, C., Snider, J., Bedri, N., Elhussein, T. A., & Elamin, S. A. (2019). The Saleema initiative in Sudan to abandon female genital mutilation: Outcomes and dose response effects. PLOS ONE, 14(3), e0213380. https://doi.org/10.1371/journal.pone.0213380
- UNFPA. (2023, March 23). Countering female genital mutilation in Sudan: “I didn’t know it was possible not to cut my daughter”. UNFPA. https://www.unfpa.org/news/countering-female-genital-mutilation-sudan-%E2%80%9Ci-didn%E2%80%99t-know-it-was-possible-not-cut-my-daughter%E2%80%9D
- World Vision International. (2023). World Vision Engages Local Protection Networks to Prevent Harmful Practices Against Children in East Darfur. https://www.wvi.org/stories/sudan/world-vision-engages-local-protection-networks-prevent-harmful-practices-against
- Ayang, P. (2024, February 27). Female Genital Mutilation Continues Amid Sudan’s Conflict and Forced Displacement. IPS. https://www.ipsnews.net/2024/02/female-genital-mutilation-continues-amid-sudans-conflict-and-forced-displacement/?utm_source=rss&utm_medium=rss&utm_campaign=female-genital-mutilation-continues-amid-sudans-conflict-and-forced-displacement#google_vignette
- UNHCR. (2024, June). Factsheet—Egpyt: June 2024. https://data.unhcr.org/en/documents/details/109505
- UNHCR. (2024). Egypt: Sudan Emergency Response Update #39. https://data.unhcr.org/en/documents/details/111511
- UNHCR. (2024). Emergency Response—New Arrivals from Sudan (UNHCR Comprehensive Overview of Response to Emergencies). https://data.unhcr.org/en/documents/details/111634
- UNHCR. (2024, September 24). Overview of Refugees and Asylum-seekers in Egypt. Egypt: Population Dashboard. https://app.powerbi.com/view?r=eyJrIjoiZGIxNDIwMWUtMjIwYS00YjIyLWFhMTgtMWJhNzNkNDkyNjM5IiwidCI6ImU1YzM3OTgxLTY2NjQtNDEzNC04YTBjLTY1NDNkMmFmODBiZSIsImMiOjh9
- Creta, S., & Khalil, N. (2024, April 25). EXCLUSIVE: Inside Egypt’s secret scheme to detain and deport thousands of Sudanese refugees. The New Humanitarian. https://www.thenewhumanitarian.org/investigations/2024/04/25/exclusive-inside-egypt-secret-scheme-detain-deport-thousands-sudan-refugees
- Hendawi, H., & Ahmed, A. S. (2024, July 2). Egypt toughens approach to Sudanese migrants as it cracks down on illegal migration. The National. https://www.thenationalnews.com/news/mena/2024/07/02/egypt-toughens-approach-to-sudanese-migrants-as-it-cracks-down-on-illegal-migration/
- The New Humanitarian. (n.d.). A Sudanese collective’s care in Cairo | First Person [Broadcast]. https://www.youtube.com/watch?app=desktop&v=FuC5-2fmkSo
- Barrett, H. R., Bedri, N., & Krishnapalan, N. (2021). The Female Genital Mutilation (FGM) – migration matrix: The case of the Arab League Region. Health Care for Women International, 42(2), 186–212. https://doi.org/10.1080/07399332.2020.1789642
- D’Odorico, G., Hossain, M., Jamal, E., Scarpassa do Prado, D., Roberts, C., & Palmer, J. (2021). The gender-based violence (GBV) situation and response in Cabo Delgado, Mozambique: A rapid assessment. London School of Hygiene & Tropical Medicine and United Nations Refugee Agency.
- Elnakib, S., Paina, L., Attal, B., Akter, R., Khoury, G., Karim, L., Barkat, H. H., Tamang, A., Yenokyan, G., Metzler, J., & Robinson, C. (2023). Incidence of child marriage among refugees and internally displaced persons in the Middle East and South Asia: Evidence from six cross-sectional surveys. BMJ Open, 13(6), e070056. https://doi.org/10.1136/bmjopen-2022-070056
- Elnakib, S., Hussein, S. A., Hafez, S., Elsallab, M., Hunersen, K., Metzler, J., & Robinson, W. C. (2021). Drivers and consequences of child marriage in a context of protracted displacement: A qualitative study among Syrian refugees in Egypt. BMC Public Health, 21(1), 674. https://doi.org/10.1186/s12889-021-10718-8
- Mitike, G., & Deressa, W. (2009). Prevalence and associated factors of female genital mutilation among Somali refugees in eastern Ethiopia: A cross-sectional study. BMC Public Health, 9(1), 264. https://doi.org/10.1186/1471-2458-9-264
- Ryan, M., Glennie, A., Robertson, L., & Wilson, A.-M. (2014). The Impact of Emergency Situations on Female Genital Mutilation (28 Too Many Briefing Paper). https://www.fgmcri.org/media/uploads/What%20is%20FGMC/the_impact_of_emergency_situations_on_fgm.pdf
- Chadha, M. (n.d.). Catastrophic Ramifications of Armed Conflicts on Women. International Journal of Law Management & Humanities, 4(6), 788–797. https://doij.org/10.10000/IJLMH.112332
- Amnesty International. (2004). Lives blown apart: Crimes against women in times of conflict: Stop violence against women. https://www.amnesty.org/en/wp-content/uploads/2021/08/act770752004en.pdf
- Plan International. (2023). Female genital mutilation/cutting: Policy brief. https://plan-international.org/uploads/2023/02/GLO-FGMC_Policy_Brief-FINAL-io-ENG-jan23.pdf
- Salih, Z. M. (2016, February 15). FGM spreading to minority groups in Sudan, say campaigners. The Guardian. https://www.theguardian.com/world/2016/feb/15/fgm-sudan-female-genital-mutilation-spreading
- Nielsen, N. (2017, September 25). Syrians find troubled homes in Egypt. EUobserver. https://euobserver.com/eu-and-the-world/ar8a27d624
- Simojoki, M. V. (2014). Female Genital Mutilation—Practices Amongst the Refugee Population in Upper Nile State, South Sudan. The Danish Refugee Council. https://data.unhcr.org/en/documents/details/29215
- SAT-7 UK. (2015, July 31). Needle and Thread Exposes Racism in Egypt. SAT-7 UK. https://www.sat7uk.org/needle-and-thread-exposes-racism-in-egypt/
- UNICEF. (2022). Female Genital Mutilation in Sudan—Factsheet.
- Izugbara, C., Muthuri, S., Muuo, S., Egesa, C., Franchi, G., Mcalpine, A., Bacchus, L., & Hossain, M. (2020). ‘They Say Our Work Is Not Halal’: Experiences and Challenges of Refugee Community Workers Involved in Gender-based Violence Prevention and Care in Dadaab, Kenya. Journal of Refugee Studies, 33(3), 521–536. https://doi.org/10.1093/jrs/fey055
- Palmer, J., Sokiri, S., Char, J. N. B., Vivian, A., Ferris, D., Venner, G., & Dak, J. J. (2024). From humanitarian crisis to employment crisis: The lives and livelihoods of South Sudanese refugee health workers in Uganda. The International Journal of Health Planning and Management, 39(3), 671–688. https://doi.org/10.1002/hpm.3777
- Afifi, M. (2009). Women’s empowerment and the intention to continue the practice of female genital cutting in Egypt. Archives of Iranian Medicine, 12(2), 154–160.
- Ameyaw, E. K., Anjorin, S., Ahinkorah, B. O., Seidu, A.-A., Uthman, O. A., Keetile, M., & Yaya, S. (2021). Women’s empowerment and female genital mutilation intention for daughters in Sierra Leone: A multilevel analysis. BMC Women’s Health, 21(1), 200. https://doi.org/10.1186/s12905-021-01340-2
- Doucet, M.-H., Delamou, A., Manet, H., & Groleau, D. (2020). Beyond will: The empowerment conditions needed to abandon female genital mutilation in Conakry (Guinea), a focused ethnography. Reproductive Health, 17(1), 61. https://doi.org/10.1186/s12978-020-00910-1
Authors: This brief was written by Meral Marouf (UNICEF MENA, [email protected], ORCID 0009-0007-8267-8745) and Jennifer Palmer (London School of Hygiene & Tropical Medicine, LSHTM, [email protected], ORCID 0000-0001-7777-722X).
Acknowledgements: Input was received from a range of experts: Salma Samy (Care Egypt), Mohamed Abdellatif and Marwa Moawad (both from Save the Children – Aswan office), Enaam Mohamed and Alaa Salah (both from Sanad Safe Space), and Naglaa Mehana (Etijah). The brief was reviewed by Nasifa Bedri (Ahfad University for Women, Sudan), Hazel Barrett (Coventry University, UK), Engy Sawah (Institute of Tropical Medicine – Antwerp, Belgium) and Nada Mustafa Ali (University of Massachusetts Boston, USA). Editorial support provided by Georgina Roche (SSHAP editorial team). This brief is the responsibility of SSHAP.
Suggested citation: Marouf, M. and Palmer, J. (2024). Key considerations: Female genital mutilation among Sudanese displaced populations in Egypt. Social Science in Humanitarian Action (SSHAP). www.doi.org/10.19088/SSHAP.2024.059
Published by the Institute of Development Studies: October 2024.
Copyright: © Institute of Development Studies 2024. This is an Open Access paper distributed under the terms of the Creative Commons Attribution 4.0 International licence (CC BY 4.0). Except where otherwise stated, this permits unrestricted use, distribution, and reproduction in any medium, provided the original authors and source are credited and any modifications or adaptations are indicated.
Contact: If you have a direct request concerning the brief, tools, additional technical expertise or remote analysis, or should you like to be considered for the network of advisers, please contact the Social Science in Humanitarian Action Platform by emailing Annie Lowden ([email protected]) or Juliet Bedford ([email protected]).
About SSHAP: The Social Science in Humanitarian Action (SSHAP) is a partnership between the Institute of Development Studies, Anthrologica , CRCF Senegal, Gulu University, Le Groupe d’Etudes sur les Conflits et la Sécurité Humaine (GEC-SH), the London School of Hygiene and Tropical Medicine, the Sierra Leone Urban Research Centre, University of Ibadan, and the University of Juba. This work was supported by the UK Foreign, Commonwealth & Development Office (FCDO) and Wellcome 225449/Z/22/Z. The views expressed are those of the authors and do not necessarily reflect those of the funders, or the views or policies of the project partners.
Keep in touch
Email: [email protected]
Website: www.socialscienceinaction.org
Newsletter: SSHAP newsletter

