
This brief summarises key considerations concerning cross-border dynamics between Uganda and Rwanda in the context of the 2022 outbreak of Ebola (Sudan Virus Disease, SVD) in Uganda. It is part of a series focusing on at-risk border areas between Uganda and four high priority neighbouring countries: Rwanda; Tanzania; Kenya; and South Sudan.
The outbreak began in Mubende, Uganda on 19 September 2022, approximately 300 kilometres from the Uganda-Rwanda border. At the time of writing (November 2022) it has spread to nine Ugandan districts, including two in the Kampala metropolitan area. Kampala is a transport hub, with a population over 3.6 million. While the global risk from SVD remains low according to the World Health Organization, its presence in the Uganda capital has significantly heightened the risk to regional neighbours. Rwanda is categorised as Priority 1, with significant preparedness activities underway.
As of November 2022, there had been no case of SVD imported from Uganda into Rwanda, although alerts have been triggered at border posts. This brief provides details about cross-border relations, the political and economic dynamics likely to influence these, and specific areas and actors most at risk. It is based on a rapid review of existing published and grey literature, news reports, previous ethnographic research in Rwanda and Uganda, and informal discussions with colleagues from Save the Children, UNICEF, UNECA, UNDP, IOM, TBI, and the World Bank. It was requested by the Collective Service, written by Hugh Lamarque (University of Edinburgh) and supported by Olivia Tulloch (Anthrologica. It was reviewed by colleagues from Save the Children, Anthrologica, the Institute of Development Studies and the Collective Service. This brief is the responsibility of SSHAP.
Key Considerations
- Border and border crossings: The Uganda – Rwanda border is 169km long, with few natural barriers and three official crossing points. Crossing points at Katuna-Gatuna and Mirama Hills-Kagitumba are connected to Kampala via major highways. A crossing point at Kyanika – Cyanika may be less directly connected to the SVD epicentres in Uganda, but introduces the additional economic risk of an outbreak close to Musanze, which would be especially damaging for Rwanda’s gorilla tourism industry.
- Long distance trade and transport pose a risk of transmission, which increased significantly with the spread of SVD to the Kampala metropolitan area. Approximately 50-80 freight vehicles and 10-20 long distance bus services cross the border per day.
- High-risk districts: The government of Rwanda has identified eight districts at high risk of SVD transmission: the three districts of the capital Kigali and all districts that make contact with Ugandan territory. All border districts report high rates of household communication devices (phones and radios) and high uptake of community-based health insurance (Mutuelle de Santé). All districts have been exposed to prior EVD sensitisation campaigns, most notably during the 2018-2020 Ebola outbreak in the DRC.
- Border region and cross-border movement: There have been no cases of SVD in the border region to date. No large urban districts make contact with the border. Countryside population densities are however very high. Midsize towns of Kabale and Kisoro in Uganda and Musanze, Byumba, and Nyagatare in Rwanda act as regional markets that draw cross-border trade. Informal cross-border trade is common practice, with daily border crossers estimated in the low thousands.
- State Preparedness: Rwandan state authorities are well-prepared for an SVD outbreak. This includes a standard operating procedure for nutrition, in cases where livelihoods and sources of income are disrupted by disease control measures. In October 2022 the WHO categorised Rwanda as the most prepared for an SVD outbreak of all priority 1 and priority 2 countries. Suspicion of external interventions makes it particularly important that international response actors undertake early and sustained dialogue with national authorities to avoid misunderstandings and duplicated efforts.
- Community engagement: Outreach to communities is facilitated by a fine-grained system of decentralisation down to the level of small neighbourhoods. Local associations (e.g. women’s trading cooperatives and motorbike taxi associations) are tightly organised. They are accessible through the state and can be used to counter concerns emerging from social listening data. International response actors should work through these existing mechanisms.
- Healthcare response: The Rwandan government is highly autonomous and capable of implementing its own Ebola prevention measures. An Ebola Taskforce includes twenty-three agencies and is co-chaired by the Minister of Health and the WHO. An Ebola Treatment Centre has been established at Nyamata Hospital in Bugasera, equipped with 134 isolation beds. Ebola testing sites have been set up at major hospitals.
- Border closures: The border with Uganda has recently been reopened for the first time since February 2019. The practicalities of closing the border are well established and could be conducted quickly. If so, contingency planning would be necessary to ensure that border communities are safeguarded against the removal of their survival economy in cross-border trade.
- Conflict in the Democratic Republic of Congo (DRC): Conflict in neighbouring DRC has escalated significantly in recent weeks. The security situation is characterised by secrecy, paranoia, and non-cooperation between states, all of which complicate effective disease control measures. Border-crossings, legal and illegal, are sensitive sites managed by the armed forces who may be reluctant to share information, particularly if it is seen to pertain to national security.
- Refugees: Recent violence in the DRC has displaced approximately 240,000 people. Since October 2022 thousands of refugees have been registered crossing the Bunagana border post and entering southern Uganda close to the Rwandan border. These populations are at greater risk of SVD transmission due to their high mobility and tendency to avoid authorities including healthcare workers.
- Language: Kinyarwanda is the dominant language in the districts of northern Rwanda. It should be the main language of disease risk communication and engagement with communities on the Rwandan side of the border. Southern Uganda is more linguistically diverse. Kiga (also known as Rukiga, Ruchiga, or Chiga) is the most commonly spoken language in Kisoro and Kabale and response teams should have capacity to communicate in these languages. The national languages Luganda and English are also commonly understood.
Border region and physical terrain
The Rwanda-Uganda border is short, at 169 kilometres. It stretches from a tri-border point with the Democratic Republic of Congo (DRC) in the west, to a tri-point with Tanzania at the River Kagera in the east. The westernmost point is on the summit of Mount Sabyinyo, and the western 15 kilometres of the border run up steep forested slopes inside the Volcanoes National Park.
Other than the mountainous terrain in the far west, and a short section of the Muvumba river in the east, the border contains no natural barriers, and is demarcated based on territory associated with particular hillslopes. The result is a complicated, meandering borderline, designated by intermittent border markers.
There are three official crossing points: Cyanika (Rwanda) – Kyanika (Uganda) in the west; Gatuna (Rwanda) – Katuna (Uganda) towards the centre; and Kagitumba (Rwanda) – Mirama Hills (Uganda) in the east close to Tanzania.
The Ugandan town of Kabale acts as a central market and transport hub in the south of Uganda, where residents have a high degree of interaction across the Gatuna-Katuna border post into Rwanda.
| Regional map with road connections Border region with major crossing points |
 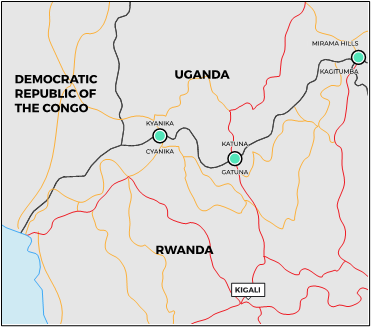 |
Source: Author’s own
Long distance trade and transport
At present, the highest risk of cross-border transmission stems from long-distance trade and transport into Rwanda. This risk has been significantly heightened by the presence of SVD in the Kampala metropolitan area, which is linked directly by road to the border posts of Katuna (Uganda) – Gatuna (Rwanda) and Mirama Hills (Uganda) – Kagitumba (Rwanda).1
Kigali is considered at risk due to the high-quality transport infrastructure that links it to border areas, its international airport, and the possibility that people with SVD symptoms from other districts may travel to the capital to seek medical care. The city is approximately 1.5 hours by car from Gatuna and 4.5 hours from Kagitumba. Cases in the Ugandan towns of Masaka or Mbarara (on the road between Kampala and the border) would heighten concerns about cross-border risk and suggest the virus is moving along the trade route. There is no reason, however, why the disease could not bypass these towns and arrive directly in Rwanda. Most long-distance transport through the border is destined for Kigali, and it is likely that if SVD arrives by this means into Rwanda, its first contacts will be in the capital.
Based on figures from recent years (excluding the COVID-19 pandemic), up to 2,500 freight vehicles cross the border each month, an average of just over 80 per day, with most containing two persons (driver and assistant).2 The majority will have passed through Kampala, staying close to the capital for rest, refuelling, and loading and unloading of goods. Freight arriving along the Northern Corridor, which connects Kigali with Kampala, Nairobi, and the port of Mombasa, is likely to be destined either for Kigali, or for the Congolese hub cities of Goma and Bukavu, transiting large sections of Rwandan territory.3 While the numbers are relatively low, these vehicles introduce the possibility of long distance transmission for SVD and should be monitored appropriately.
Regular bus services, with nine arrivals per day, link Kampala and Kigali, a distance of 510 kilometres that takes between eight and ten hours to drive. These vehicles include 22-person capacity Toyota Coasters, as well as larger coaches with capacities up to 60. Two coaches per day arrive from Nairobi, having stopped on route in Kampala. These numbers amount to approximately 400 arrivals per day and do not include private vehicles on the same road.
Regular temperature screening and handwashing are taking place at all Rwandan points of entry, and test centres have been established in close proximity to them. Border officers and health workers have been trained to monitor passengers arriving from the SVD epicentres in Kassanda and Mubende districts (where Ugandan authorities have also instigated a travel ban).
Cross-border community transmission
Cross-border community transmission presents unique difficulties in terms of disease control. At present the risk remains low. So far, no SVD cases have been reported in the Uganda border districts of Kisoro, Rubanda, or Kabale. On 22 October 2022, one probable case alert was triggered in Ntungamo, with the patient evacuated successfully.4 Ntungamo district shares a small stretch of border with Rwanda, but the case was reported in the district capital, 34 kilometres from Mirama Hills border post. Twelve contacts were identified and none have shown symptoms. Ntungambo is not currently listed as a priority district by Ugandan authorities.
In the event that community spread of SVD is detected in these districts, the following considerations are relevant:
- The border region is predominantly rural, without any large urban spaces directly contacting it. The three official border crossings: 1) Kyanika (Uganda) – Cyanika (Rwanda); 2) Katuna (Uganda) – Gatuna (Rwanda); and 3) Mirama Hills (Uganda) – Kagitumba (Rwanda) are surrounded by relatively small municipalities on both sides of the border, each with combined populations in the hundreds or low thousands.
- Rural districts close to the border are nonetheless densely populated. Rwandan territory as a whole is the most densely populated in continental Africa with approximately 525 people per square kilometre, raising the risk of community transmission in the countryside.5
- The border sees a significant degree of informal cross-border trade, notably in foodstuffs. Not all traders make use of official crossing points. In October 2022, the Rwandan government screened 15,329 people at border crossings, approximately 500 per day.6 The total number of border crossers is likely to be significantly higher, especially if it includes informal traders crossing on foot, who may be screened with handheld temperature scanners but are not formally registered in screening statistics. In the event that SVD cases emerge close to the border, Rwandan authorities are likely to scale up screening and crack down more strongly on informal and illegal crossing points.
- A 2018 study showed a high rate of cross-border mobility linked to healthcare seeking on the Uganda-Rwanda border. The majority of respondents (83.9%; 234/279) had accessed care from public health facilities. Nearly one-third (77/279) had sought care across the border more than a year ago and 22.9% (64/279) less than a month ago.7 If this trend has re-emerged following the 2019-2022 border closure, it would suggest a heightened risk of cross-border care seeking from persons at risk from SVD.
State preparedness and disease control in recent history
Rwandan state authorities are well-prepared for an SVD outbreak, having drawn valuable experience from the 2018-2019 EVD outbreak in neighbouring DRC and from the prolonged implementation of strict lockdown measures during the height of the COVID-19 pandemic. The preparedness measures include a standard operating procedure for nutrition, in cases where livelihoods and sources of income are disrupted by disease control measures. An operational readiness report from the WHO in October 2022 ranked Rwanda the most prepared of the priority 1 and priority 2 countries, in the context of the SVD outbreak in Uganda.
The Rwandan government is highly autonomous and capable of implementing its own Ebola prevention measures through the Ministry of Health (MoH), Ministry of Local Government (MINALOC), Rwanda Health Communication Centre (RHCC), and the Rwanda Biomedical Centre (RBC). These groups are supported by the Rwanda Defence Force (RDF) and the Rwanda National Police (RNP). An Ebola Taskforce was established at the national level following the announcement of the 2018 outbreak in DRC. It includes twenty-three agencies and is co-chaired by the Minister of Health and the WHO. It has been reactivated in response to the current SVD outbreak.
Powerful means of surveillance (patrols, community surveillance, checkpoints etc.) are already in place on both sides of the border and could be operationalised for contact tracing and active case detection if necessary. This is particularly true in Rwanda, where village communities are closely monitored and coordinated by central authorities through a sophisticated system of administrative decentralisation.8
Ebola prevention measures in Rwanda have a significant funding gap of US$11.4 million according to the WHO.9 Ongoing operational challenges include a lack of direct experience of previous Ebola outbreaks on Rwandan territory, incomplete screening at points of entry (POEs), a lack of equipment (lab gloves, thermos scanners, additional personal protective equipment (PPE) hoods), and the limited capacity at the country’s one Ebola Treatment Unit (135 beds at a facility in Nyamata, Bugasera District).10
Border closures
Due to a high-level political dispute, the Uganda-Rwanda border was closed on 27 February 2019. With the exception of transiting freight vehicles, the Rwandan government prohibited Ugandan and Rwandan nationals from crossing the border other than in exceptional circumstances. This created a temporary livelihood crisis in border districts where residents relied on cross-border trade.11 The closure was enforced, at times forcefully, by Rwandan security forces. This situation extended through the COVID-19 crisis, and the border only formally reopened in January 2022.12
Figure 1. Timeline of previous outbreaks and border closures and control measures

Source: Author’s own
The recent extended closure has a number of repercussions:
- At a practical level, Rwandan authorities will not have difficulty repeating the process of closing the border if the need arises. The actors, procedures, and technologies required to do so are already in place and have been fine tuned in recent years. Following the COVID-19 pandemic, closing borders to prevent the spread of disease has become more normalised in international relations and has lost some of the stigma it previously carried among international development actors.
- At a political level, closing the border is undesirable. Its closure in 2019 was a punitive measure, and to repeat the process now that cross-border relations have stabilised risks setting-back years of negotiations. It also sends a message that the Rwandan authorities do not have confidence in Uganda’s ability to control the current outbreak, a politically damaging sentiment. Government authorities are aware of the human suffering caused by recent closures and lockdowns to borderland communities in the north, and would prefer not to inflict the same harm again if it is preventable by other means.
- Contingency planning to mitigate the potentially destabilising effect of such a closure is required nonetheless, particularly in terms of the timely supply of foodstuffs to communities in a state of lock down, the disruption to the ‘survival economy’ for tens of thousands of residents, and the potential to force informal traders to less regulated crossing points outside the major cities on the border.
Tourism and reputational harm
Concerns about the loss of tourism revenue may influence Rwandan policy making on SVD control measures. Rwanda’s north-west region forms the backbone of the country’s tourism industry, especially the luxury travel sector that has developed around gorilla trekking in the Volcanoes National Park. While the major highways that pass through Gatuna-Katuna and Kagitumba-Mirama Hills both bypass this region, the crossing point at Cyanika-Kyanika leads directly into the district of Musanze, and through the district capital of the same name – the launching point for gorilla treks.
The development of the tourism sector has become central to government finance (representing about 10% of national GDP), and authorities will be conscious of the reputational damage even a single SVD case may lead to.13 A case in Musanze would constitute a worst-case scenario in these terms, a fact that may influence decision-making around closing the land border if the threat is seen to increase.
Insecurity and refugees
The current SVD outbreak in Uganda has a backdrop of fraught relations between Rwanda and Uganda, and Rwanda and DRC. Fighting between the March 23rd Movement militia (M23) and the Congolese Army (FARDC), backed by UN peacekeepers from the United Nations Stabilisation Mission in Congo (MONUSCO), has been intense in recent months. The conflict has centred around the regions of Rutshuru and Nyiragongo, with M23 forces controlling significant sections of territory on the Congolese side of the Rwanda-Uganda-DRC border triangle, including the Congolese border posts at Kitagoma and Bunagana.14
Since 20 October 2022, the conflict has significantly intensified, with implications for disease control measures in the Uganda – Rwanda borderland:15
- The conflict is a sensitive diplomatic topic with a history dating back to regional inter-state wars is the 1990s and early 2000s.16 Rwanda and Uganda have both been accused of arming and supporting M23 in its campaign on Congolese soil, accusations that both states deny. The conflict has raised the political profile of the border region and seen deteriorating relations between Rwandan and Ugandan authorities on the one hand, and DRC authorities on the other.
- State security forces in the border areas are on high alert, in precaution against the conflict spilling over into Rwanda or Uganda, or the situation escalating into inter-state war. High profile border security incidents are becoming more regular occurrences, most recently including the violation of Rwandan airspace by Congolese military aircraft.17 The heightened security presence means that all states involved have a significant coercive and logistical capacity at their disposal, which could in theory be diverted to disease prevention if the SVD outbreak reaches the area. However, the security situation is characterised by secrecy, paranoia, and non-cooperation between states, all of which complicate effective disease control measures. Border-crossings, both legal and illegal, are sensitive sites managed by the armed forces who may be reluctant to share information, particularly if it is seen to pertain to national security.
- A recent surge in violence in DRC since 20 October 2022 has displaced at least 188,000 people, bringing the total displaced by the crisis to approximately 300,000.18 These numbers change on a daily basis, but as an indication of the scale of movement, 12,000 refugees were registered crossing the Bunagana border post and entering southern Uganda in just four days between 22 October and 26 October.19 Many remain unhoused, sheltering among host communities and in the Bunagana school. Others were first moved to Nyakabanbe transit centre in Kisoro, which has since been closed for security and sanitation reasons, and then further north to Nyakivale.20 The influx of refugees into both Rwanda (at Rubavu) and Uganda (at Bunagana and into Kisoro) adds a layer of complexity to contingency planning for an SVD outbreak, given the increased mobility of the population and the limited sanitation in temporary housing and refugee transit centres.
Socio-Political Context in Northern Rwanda
In response to the SVD outbreak, the government of Rwanda has identified eight high risk districts (see map). These include the three districts that make up the capital Kigali (Nyarugenge, Gasabo, and Kicukiro), as well as all districts that border with Ugandan territory (Rubavu, Nyabihu, Musanze, Burera, Gicumbi, and Nyagatare).
Map showing districts at high risk of SVD
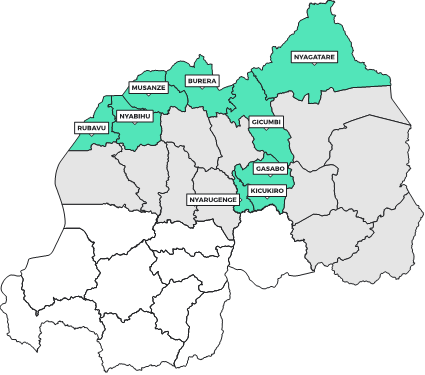
Source: Author’s own
Existing data from the 2012 national housing census show the district population on the northern border to range between 350,000 and 450,000, for a total borderland population of approximately 2.4 million (roughly 20% of the national population). These border districts house four medium-sized Rwandan cities with populations between 50,000 and 100,000 people: Rubavu (Rubavu district on the DRC border), Musanze (Musanze district), Byumba (Gicumbi district), and Nyagatare (Nyagatare District).
Key demographic factors in priority districts
Rwanda is a small, densely populated state with a strong internal system of administrative decentralisation. While urban centres (especially Kigali) tend to be wealthier than rural regions, there is not the same degree of inter-district variation in health, poverty, and developmental indicators that can be found in the country’s larger regional neighbours. The terrain is one of steep hills, and road access can at times be restricted, especially during the rainy seasons (March-May and September-November). Nevertheless, the small size of the country means very few areas can be considered entirely remote or disconnected from central administration.
Drawing on 2019/2020 District Surveys conducted by the Rwandan National Institute from Statistics certain key statistics have relevance for SVD preparedness.21,22,23
- Rural households in northern Rwanda have good access to communication devices. Of the six priority districts, approximately 30-40% of individual households had a radio, 10% had a television and 60-70% had a mobile phone (Table 2). Radio use was shown to be very high in rural regions, with 80-90% of the population having listened to radio broadcasts within one week of the survey (Table 1). Combined with regular in-person community meetings and a high population density, these numbers suggest that sensitisation to disease symptoms, spread and control measures can be conducted effectively on a large scale.
- Border populations, for the most part, showed a high degree of access to handwashing places (Burera district being an outlier with lower rates). Most people (85-95%) had access to either mobile or fixed handwashing places, although the majority were mobile (Table 3). These numbers – already high to begin with – are likely to have increased significantly in the aftermath of COVID-19 preventative measures.
- Universal health insurance initiatives (mutuelle de santé) have been extremely effective in terms of uptake, with 85-95% of Rwandans covered in the key districts. This significantly reduces the risk that patients avoid health facilities for financial reasons.
- In response to a knowledge, attitudes, and practice (KAP) survey conducted in October 2018, the majority of respondents (93%) confirmed that they would go to a health centre as their primary point of contact with the health system if they thought they may have Ebola (with over 85% saying they would do so within a day or two).24
| Table 1. % of men and women who listen to radio at least once a week | ||
| Men aged 14-49 | Women aged 14-49 | |
| Rwanda National Average | 80 | 62 |
| Rubavu | 74 | 67 |
| Nyabihu | 87 | 60 |
| Musanze | 93 | 70 |
| Burera | 75 | 44 |
| Gicumbi | 69 | 45 |
| Nyagatare | 70 | 65 |
Source: Author’s own table, drawn using raw data publicly available from NISR (2020). Demographic and Health Surveys, 2019/2020, Western, Eastern, and Northern Province Profiles.
Local administration
Administrative decentralisation in Rwanda extends down to the local level, where every 100-150 Rwandan households, the umudugudu (plural imidugudu), elects a leader who chairs a Community Policing Committee (CPC) of five members.25 These groups meet regularly to discuss incidents of note within the neighbourhood, and serve as a powerful means of gathering and disseminating information regarding Ebola preparedness and prevention.
Each umudugudu generally hosts at least one community health worker, a valuable point of contact for the response. It is routine procedure that every morning, reports from imidugudu are passed up to cell (akagari) authorities (approximately 50-100 neighbourhoods), often via WhatsApp, and then onwards to the sector (umurenge), district (akarere) and national level, where a meeting of the Joint Operations Centre (JOC) is convened daily in Kigali to discuss serious incidents that have occurred throughout the country over the previous 24 hours.
The oversight of medical services has also been decentralised to the district level and is managed from district headquarters across the country. This infrastructure could be adapted to perform contact tracing, surveillance and active case detection should there be an outbreak of SVD in Rwanda. The access that external Ebola response partners would have to these networks may be limited, however, and dependent on good relations with the Rwandan central government and its security forces.
In general, the Rwandan Defence Force is suspicious of outside interventions, an attitude that can be traced back to international inaction during the 1994 Genocide against the Tutsi. The security services are likely to act independently of international actors in their preparedness and prevention efforts. International response actors would benefit from an early and sustained dialogue with national authorities to avoid misunderstandings and duplicated efforts, and to improve coordination and collaboration.
Local associations and community outreach
Community engagement needs to take place not only at the border itself, but also within the wider borderland community that is located further from the immediate border posts. On the Rwandan side, community engagement measures continue to be implemented by the Government of Rwanda with the support of partners including UNICEF and International Committee of the Red Cross (ICRC). Radio is used by the majority of local residents to receive key information.
A recent social media study on the Uganda SVD outbreak (1 – 7 November 2022) identified recurring narratives in the region that can be addressed through effective community engagement and outreach: 26
- Concerns about ‘’safe and dignified burial practices’’
- Speculation about unverified cures for the disease.
- Suspicion about SVD related deaths taking place in government facilities.
- Questions over transmission, and specifically whether SVD is an airborne disease.
- Claims that Ebola is a business and a driver of corruption.
Rwanda’s sophisticated system of administrative decentralisation means that channels are already in place through which information can be readily disseminated to the population at large. Such interactions require the approval of central authorities at MINALOC, the RNP and the President’s Office, and positive coordination is key to ensuring consistent messaging and a coherent response. Demonstrating accountability to the needs of the community and acting on community feedback will reduce scepticism associated with outside actors.
Business and civil society associations will likely be most effectively accessed through the state, and in particularly through government authorities at the district level. Linking up with local associations is important due to their extensive geographic reach and social embeddedness, and the fact that they tend to be trusted by their members. Such associations include transport associations (bus, truckers, taxis, or motorbike taxis), trade associations, money exchange associations at the border, and traditional healer associations. Many of these groups have sophisticated internal hierarchies that allow points of contact for external actors, either through elected regional heads or spokespersons. Establishing mechanisms for sustained dialogue is key, as is emphasising flexibility based on local feedback.
Women make up the majority of cross-border traders, and women’s trade cooperatives are an extremely valuable point of access for both disseminating and gathering information. Throughout the borderland, markets are important sites for meeting and reinforcing connections as well as for trade, community engagement and the introduction of routine protection mechanisms such as handwashing stations.
Language
Districts of northern Rwanda share Kinyarwanda as the first language spoken by the overwhelming majority of the population and it should be the main language of the disease response and sensitisation campaign on the Rwandan side of the border. English is commonly spoken among an urban middle class and younger generations, while French is spoken in districts bordering DRC – notably Rubavu and Nyabihu – and among an older generation. Swahili is commonly understood, and used as a trading language, particularly among Bantu-language speakers from elsewhere in the region. Speaking Kinyarwanda is often an identifying marker – at times negatively – and Rwandans may be reluctant to speak it outside of Rwanda to avoid discrimination.
Southern Uganda is more linguistically diverse. Kiga (also known as Rukiga, Ruchiga, or Chiga) is the most commonly spoken language in Kisoro and Kabale. The national languages Luganda and English are also commonly understood. French is spoken by Ugandans living close to the DRC border. While Swahili is used as a trading language with other Bantu language speakers, it has been known to carry stigma in Uganda, as the language of the military during periods of military rule in Uganda. Refugee populations in the region may speak a range of indigenous Congolese languages, but are most likely to communicate in Congolese Swahili and French.
Healthcare System and Ebola Response
In early 2020, Rwandan authorities were able to effectively adapt emergency measures intended for Ebola and repurpose them to address the risks associated with COVID-19. These measures are now being once again adapted to the new threat of SVD – and a significant amount of preparation in terms of facilities, outreach, and trainings, has already taken place.
Rwanda has a shortage of healthcare professionals with approximately 1.3 medical doctors per 1,000 people. This limits the country’s overall capacity to respond to an epidemic. The government is committed to strengthening its quality of service through a bottom-up approach, and in the current administrative system, each village elects three volunteers to act as Community Health Workers for the general population (one man and one woman for general diseases, and another woman for maternal and antenatal care). These volunteers act as ‘the first line of defence’ and are trained to address 80% of the burden of disease through home-based care. The MoH has trained over 20,000 Community Health Workers to monitor health at the village level and to refer patients to the nearest health centre as required. At a health centre, cases can either be treated directly or referred onwards for more specialised care in the next tier of health facilities or a Referral Hospital.
On 12 October 2022, the WHO called a high-level emergency ministerial meeting on cross border collaboration for preparedness and response to SVD in Kampala. Rwanda, Burundi, DRC, Liberia, Sierra Leone, South Sudan, Tanzania, and Uganda were all represented. The SVD response in Rwanda has since been significantly scaled-up:27,28
- Rwanda has received WHO support on procurement of mobile Ebola Treatment Units, the deployment of experts in IPC, case management, and contact tracing, as well as support in conducting SIMEX.
- Rwanda requested a six-week bundle of additional PPE from the WHO in mid-October, and has distributed it to health centers in northern districts.
- An Ebola Treatment Centre has been established at Nyamata Hospital in Bugasera, equipped with 134 isolation beds.
- Ebola testing sites have been set up at major hospitals in Rwamagana, Rubavu, Musanze, Kibuye, CHUB (Huye), Nyarugenge, and Gihundwe.
- Regular retreats are being run to train healthcare workers and community volunteers.
- Ebola simulation exercises have been conducted at the Kigali international airport (1 November 2022) and at the Kigali King Faisal Hospital. Similar clinical drills have taken place at district hospitals across the country.29
- An Ebola prevention booth has been set up at the Gatuna border post.
- Between 1 and 31 October, 15,329 people were screened at Rwandan border crossings, and 2,200 screened at the Kigali airport. This triggered 71 alerts although to date there remain no confirmed cases of SVD in the country.
- While no vaccine has been effectively trialed against the Sudanese Ebola variant, over 200,000 Rwandans have been vaccinated against the Zaire strain of EVD, particularly in the North West. Vaccine-roll-out mechanisms are well established and the country continues its vaccination campaign, prioritizing front-line healthcare workers.
In terms of the response structure, there are currently seven technical working groups (risk communication and community engagement (RCCE); surveillance, points of entry and laboratories; logistics; vaccines; infection prevention control case management; and leadership and coordination) reporting every week to the Emergency Operations Centre (EOC) meeting.
The RCCE working group has taken extensive measures to disseminate information regarding Ebola and prevention strategies to the Rwandan population, particularly residents of the eight priority high-risk districts. Supported by response partners including UNICEF, these efforts have involved outreach through radio, television, digital billboards, town hall meetings, and call-in sessions with representatives of the Rwandan MoH. Two toll-free numbers (112 and 114) are available as reporting lines for suspected cases.
| Table 2. % of Rwandan households with communications devices | |||||||
| Radio Sets | Television | Mobile Telephone | Computer | ||||
| Rwanda National Average | 40.4 | 13.6 | 71 | 4.6 | |||
| Rubavu | 39.3 | 20.5 | 70.2 | 6.1 | |||
| Nyabihu | 33.7 | 6.7 | 71.6 | 1.3 | |||
| Musanze | 41.7 | 14 | 78.7 | 7.8 | |||
| Burera | 36.3 | 6.8 | 61.9 | 3.3 | |||
| Gicumbi | 34.4 | 2.8 | 55.8 | 0.1 | |||
| Nyagatare | 34.8 | 7.9 | 78.2 | 1 | |||
Source: Author’s own table, drawn on raw data publicly available from NISR. (2020). Demographic and Health Surveys, 2019/2020, Western, Eastern, and Northern Province Profiles.
| Table 3. % of de jure population where handwashing places were observed | |||
| Fixed Place | Mobile Place | Total | |
| Rwanda National Average | 11.9 | 72 | 83.9 |
| Rubavu | 5.7 | 90.3 | 95.9 |
| Nyabihu | 3.8 | 71 | 74.4 |
| Musanze | 13.5 | 77.5 | 90.9 |
| Burera | 2.7 | 48.7 | 51.3 |
| Gicumbi | 5.3 | 90.1 | 95.4 |
| Nyagatare | 15.2 | 69 | 84.2 |
Source: Author’s own table, drawn on raw data publicly from NISR. (2020). Demographic and Health Surveys, 2019/2020, Western, Eastern, and Northern Province Profiles
References
- WHO. (2022). Ebola disease caused by Sudan ebolavirus – Uganda. 10 November 2022. https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON423
- NCTTA. (2021). Northern Corridor Transport Observatory Report. 16th Edition, June 2021. https://top.ttcanc.org/uploads/attachments/cl1uunft002160jqxbhqvya1f-the-northern-corridor-transport-observatory-report-issue-no-16-june-2021-english.pdf
- Lamarque, H. (2021) Transport Corridors in Africa, Rochester, NY: James Currey
- WHO and Uganda MoH. (2022). Situation Report 32. https://www.afro.who.int/sites/default/files/2022-10/Ug_EVD_SitRep%2332.pdf
- World Bank. (2020). Population density: people per sq/km of land area, Rwanda. https://data.worldbank.org/indicator/EN.POP.DNST?locations=RW
- WHO. (2022). Operational Readiness in Priority 1 and 2 countries SVD in Uganda, 8 November 2022
- Ssengooba, F. et al. (2021). Experiences of seeking healthcare across the border: lessons to inform upstream policies and system developments on cross-border health in East Africa. BMJ open, 11(12), e045575.
- Chemouni, B. (2016). Taking stock of Rwanda’s decentralisation: changing local governance in a post-conflict environment. Third World Thematics: A TWQ Journal, 1(6), 763-778.
- WHO. (2022). (Unpublished) Operational Readiness in Priority 1 and 2 countries, SVD in Uganda, 8 November 2022.
- WHO. (2022). (Unpublished) Operational Readiness in Priority 1 and 2 countries, SVD in Uganda, 8 November 2022.
- Ashaba, I. M. and Bareebe, G. (2019). Closed borders and fighting words: Rwanda and Uganda’s deepening rift. https://africanarguments.org/2019/03/closed-border-fighting-words-rwanda-uganda-rift/
- Reuters. (2022). Rwanda re-opens border with Uganda but says grievances remain. https://www.reuters.com/world/africa/rwanda-re-opens-border-with-uganda-says-grievances-remain-2022-01-31/
- Tourism Economics. (2021). Data and Digital Platforms, Driving the Tourism Recovery in Rwanda. https://s3.amazonaws.com/tourism-economics/craft/Google_Rwanda_Final.pdf
- Ruhanamirindi, M. (2021). Rising tensions between Rwanda and DRC jeopardise prospects for peacebuilding in the Great Lakes region. https://reliefweb.int/report/democratic-republic-congo/rising-tensions-between-rwanda-and-drc-jeopardise-prospects-peacebuilding-great-lakes-region
- UNICEF. (2022). UNICEF Democratic Republic of the Congo Situation Report #3 (Upsurge of violence in Rutshuru territory): 01 to 07 November 2022. https://reliefweb.int/report/democratic-republic-congo/unicef-democratic-republic-congo-situation-report-3-upsurge-violence-rutshuru-territory-01-07-november-2022
- Stearns, J., & Vogel, C. (2015). The landscape of armed groups in the Eastern Congo.
- Reuters. (2022). Rwanda accuses Congo of fighter jet ‘provocation’. https://www.reuters.com/world/africa/dr-congo-violates-rwanda-airspace-provocation-govt-says-2022-11-07/
- USAID. (2022). Democratic Republic of Congo – Complex Emergency. 22 November 2022.
- ECHO. (2022). Uganda – New influx of refugees (DG ECHO, UNHCR) (ECHO Daily Flash of 26 October 2022). https://reliefweb.int/report/uganda/uganda-new-influx-refugees-dg-echo-unhcr-echo-daily-flash-26-october-2022
- The Monitor. (2022). UNHCR, govt to shut down Nyakabande refugee camp. https://www.monitor.co.ug/uganda/news/national/unhcr-govt-to-shut-down-nyakabande-refugee-camp-3991364
- NISR. (2022). Demographic and Health Survey 2019/2020 – Northern Province Profile. https://www.statistics.gov.rw/publication/1781
- NISR. (2022). Demographic and Health Survey 2019/2020 – Western Province Profile. https://www.statistics.gov.rw/publication/1779
- NISR. (2022). Demographic and Health Survey 2019/2020 – Eastern Province Profile. https://www.statistics.gov.rw/publication/1778
- Rwanda Ministry of Health, World Health Organization, UNICEF. (2018). Rapid Survey on Knowledge, Attitudes and Practices on Ebola Virus Disease (EVD) in Selected High Risk Zone Districts of Rwanda.
- Lamarque, H. (2020). Policing small communities: Rwandan law enforcement and the co-production of security. Politique africaine, 160(4), 113-138.
- Collective Service. (2022). Overview of Digital Social Listening Insights on Ebola November 7, 2022.
- WHO. (2022). (Unpublished) Operational Readiness in Priority 1 and 2 countries, SVD in Uganda, 8 November 2022.
- WHO and Uganda MoH. (2022). (Unpublished) Situation Report 44. https://www.afro.who.int/countries/uganda/publication/ebola-virus-disease-uganda-sitrep-44
- The New Times. (2022). Kigali Airport Conducts Ebola Preparedness Drills. https://www.newtimes.co.rw/article/2244/news/health/kigali-airport-conducts-ebola-preparedness-drills
Acknowledgements
This brief has been written by Hugh Lamarque ([email protected]). with expert inputs from Anstes Agnew, Charlotte Taylor, and Odette Ntambara. It was further reviewed by Dr Rumunu (PHEOC), Olivia Tulloch (Anthrologica), Annie Wilkinson (IDS), Rachel James (Collective Service). This brief is the responsibility of SSHAP. We also wish to acknowledge colleagues who were consulted in the development of this brief from Save the Children, UNICEF, UNECA, UNDP, IOM, TBI, and the World Bank.
Contact
If you have a direct request concerning the brief, tools, additional technical expertise or support, or should you like to be considered for the network of advisers, please contact the Social Science in Humanitarian Action Platform by emailing Annie Lowden ([email protected]) or Olivia Tulloch ([email protected]).
The Social Science in Humanitarian Action is a partnership between the Institute of Development Studies, Anthrologica, Gulu University, ISP Bukavu, the London School of Hygiene and Tropical Medicine, and the University of Juba. This work was supported by the UK Foreign, Commonwealth & Development Office and Wellcome 225449/Z/22/Z. The views expressed are those of the authors and do not necessarily reflect those of the funders, or the views or policies of the project partners.
Keep in touch
Twitter: @SSHAP_Action
Email: [email protected]
Website: www.socialscienceinaction.org
Newsletter: SSHAP newsletter
Suggested citation: Lamarque, H. (2022) Key Considerations: Cross-Border Dynamics between Uganda and Rwanda in the Context of the Outbreak of Ebola 2022. Social Science in Humanitarian Action (SSHAP) DOI: 10.19088/SSHAP.2022.044
Published November 2022
© Institute of Development Studies 2022
This is an Open Access paper distributed under the terms of the Creative Commons Attribution 4.0 International licence (CC BY), which permits unrestricted use, distribution, and reproduction in any medium, provided the original authors and source are credited and any modifications or adaptations are indicated. http://creativecommons.org/licenses/by/4.0/legalcode

