
In September 2023, an outbreak of mpox caused by the monkeypox virus (MPXV) clade Ib was reported in Kamituga, a mining region in the Eastern Democratic Republic of the Congo (DRC). More cases of mpox started to be reported across the country and in neighbouring countries in the east, including Rwanda, Uganda and Burundi.1 In February 2025, the Africa Centres for Disease Control and Prevention and the Director-General of the World Health Organization (WHO) determined that the ongoing upsurge of mpox continues to be a public health emergency of international concern (as first declared in August 2024).
Home-based care (HBC) – care provided in the private home of a person – often takes place informally for a wide range of reasons during epidemics. Home-based models of care are increasingly being explored by Ministries of Health as a strategy for managing outbreaks and providing treatment for mild forms of diseases, particularly in resource-limited settings. Reasons to implement HBC for mild forms of diseases include to provide care when there is a lack of access to or overburdened services, to prevent a risk of infection in health facilities, to accommodate people’s preferences and to empower the public when HBC is implemented in partnership with community members. Home-based models of c are for mpox should not supplant investments in the health system, but should be designed as a component of primary healthcare. Past experiences with HBC during outbreaks such as HIV and COVID-19 offer valuable lessons. However, the unique transmission dynamics of mpox – especially the risks it poses to children and those who are immunologically vulnerable in the home – require careful consideration. To date, attention has focused on infection, prevention and control (IPC) and water, sanitation and hygiene (WASH) in the home. Other aspects of mpox management and care at home also need to be considered. It is particularly important to recognise that mpox is not only a biomedical event: it is also a social phenomenon, impacting livelihoods, relationships, well-being and access to care and protection. Also, a lack of income in the absence of financial support is likely to hinder peoples’ ability to follow isolation guidance.
This brief outlines key considerations on health system requirements for safe and inclusive HBC. It also foregrounds structural constraints and socio-political dynamics shaping understandings and practices of HBC, taking into consideration local and gendered perspectives on home and caregiving. The brief also examines how ongoing funding cuts in global health, humanitarian aid and development assistance are straining the capacity of both community-based initiatives and healthcare systems, further complicating home and community-based response efforts. The focus is on Central and East Africa in particular.
The brief draws on conversations with experts and health actors active or knowledgeable in the region and outbreak, or both; the authors’ own expertise; and academic and grey literature on HBC and histories of epidemics in Central and East Africa. The brief includes two cases studies based on recent research in Uganda and the DRC.
Key considerations
Make underlying assumptions on access to health services explicit
- Make a strong case for HBC to help isolate and manage mild mpox cases. HBC can potentially alleviate pressure on health systems for mild disease. HBC can also potentially reduce the risk of infection to health workers, patients and their visitors in health facilities. Patients and carers may also prefer HBC as an alternative to under-resourced hospital care far from home. To do HBC safely, however, it is important to acknowledge that HBC for mpox requires a functioning health system (including access to referral mechanisms and care, home visit capacity from district nurses or community health workers, and surveillance teams) and support mechanisms to caregivers.
- Be aware that past experiences of health system neglect, economic precarity and socio-political exclusion can delay or deter healthcare seeking. The association of mpox caused by MPXV clade Ib with sexual transmission can lead to stigmatisation, which may exacerbate avoidance of health services, especially in legal contexts where same-sex relations and transactional sex are criminalised.
- Acknowledge that socially and politically marginalised populations are often most affected by mpox. Provide adequate support for these populations to conduct HBC, rather than merely shifting responsibility to those who are already overburdened.
Acknowledge socio-economic and political issues hindering people’s ability to follow public health guidance on HBC
- Avoid making assumptions about people’s capacity to access healthcare and support. One example is not to assume that a person has the financial ability to seek care if symptoms get severe.
- Consider the heterogeneity of living arrangements when implementing HBC. People’s capacity to protect themselves or others from getting infected with mpox may be impacted by their social arrangements, such as urban and rural communal living arrangements, high-density living (including camps for internally displaced people), mobile and cross-border livelihoods, multigenerational and single person households, and a lack of waste collection services.
- Adapt guidelines to the local realities of caregiving and consider how these impact vulnerabilities. Evidence shows that women disproportionately contribute to caregiving at home, performing unpaid and sometimes invisible labour. Gendered practices of caregiving impact women’s vulnerability to diseases and other health and social risks. Caregivers – and women in particular – may therefore benefit from a wide range of support, such as material, financial, social and mental health support.
Incorporate evidence on political histories and power dynamics to inform HBC guidelines
- Reinforce a broader conceptualisation and implementation of the ‘community protection’ agenda. Alongside protection from mpox, consider socio-economic and political vulnerabilities associated with mpox and isolation at home.
- Enhance the prevention and control of mpox in the home by using technical approaches focusing on IPC and WASH, as well as risk communication and community engagement (RCCE) activities. These technical approaches and RCCE activities have been driven by intra-household mpox transmission. Recent guidelines offer pathways to adapt safe practices in resource-constrained settings. The broader impacts of public health interventions on social, economic and human rights are important additional elements to consider.
- Balance surveillance and containment measures with protection measures, particularly in contexts of armed violence and forced displacement, and when engaging with politically marginalised people. Militarised public health responses embed soldiers in the delivery of healthcare. These responses are often perceived by politically marginalised groups as a way of entrenching authoritarian governance, whilst neglecting or criminalising vulnerable populations. When responding to outbreaks like mpox, it is vital to incorporate a conflict-sensitive lens and rights-based approach to ensure that interventions do not exacerbate existing tensions.
Use participatory approaches to tailor HBC guidelines at a subnational level
- Be aware that community health workers are often asked to respond to multiple health emergencies by different donors at the same time. This is important to consider when engaging with community health workers to design training packages on HBC.
- Use appropriate messaging for information on HBC and ensure the messaging is delivered by figures of public authority that are perceived locally to be legitimate. The HBC information should cover mpox prevention, control and clinical management, and the messaging should be appropriate for – and must reach – marginalised communities.
- Co-produce messages and interventions with those affected by mpox.
Provide multidimensional support to caregivers at home
- Provide actionable and detailed guidance on IPC and health seeking. The guidance and recommendations should cover community-based care, such as recognising symptoms early, knowing when and where to seek care, practicing self-care, identifying strategies to prevent onward transmission, and addressing stigma in communities.
- Include access to food as a component of HBC. Lack of food provision in certain health facilities and mpox transit centres has been identified as a major challenge for patients’ attendance and retention.
- Support and protect people’s livelihoods through cash transfers, and support workers with negotiating sick leave and contract extensions with employers, when possible.
- Address the psychosocial needs of mpox patients and caregivers. While isolating with mpox at home, patients and their caregivers are particularly vulnerable to psychosocial impacts from mpox. The potential stigmatisation associated with the disease and isolation at home can undermine people’s well-being. To avoid stigmatisation, healthcare and community health workers should consider wearing unbranded clothing and not arriving in an agency car when conducting supportive visits.
- Balance children’s vulnerability to mpox with risks of separation from family members. HBC as an approach can contribute to preventing separations between parents and children. Rights-based and protection-based approaches should complement biomedical and epidemiological risk assessments.
- Recognise the hidden costs of HBC. Pay particular attention to the gendered burden of care and the disruption to livelihoods caused by isolation or caring for loved ones.
Mpox epidemiological dynamics in Central and East Africa
According to a recent situational update (13 May 2025), Sierra Leone, the DRC, Uganda and Burundi accounted for 98.1% of confirmed mpox cases reported in the previous week.2 At the time of writing, the DRC continues to report the highest number of cumulative confirmed mpox cases in Africa in 2025, although reporting gaps are occurring in the eastern part of the DRC due to an escalation of conflict and extensive funding cuts since early 2025.3 Nevertheless, MPXV clade Ia and Ib continue to circulate in the country.3 Although decreasing, the incidence of MPXV clade Ib mpox cases in Uganda continues to be high at the time of writing, while Sierra Leone is reporting a surge in confirmed mpox cases (MPXV clade IIb, with genomic testing underway). Meanwhile, Burundi, which experienced a large MPXV clade Ib mpox outbreak during the first half of 2024 and early 2025, has reported fewer cases since February 2025.
The WHO defines community transmission as being ‘if at least one case reported during the last six weeks has no epidemiological link to travel or contact with a traveller from a country with known mpox transmission. This classification applies regardless of the total number of cases reported’.3 Within Africa, community transmission of MPXV clade Ib has also been reported in Kenya, Malawi, the Congo, Rwanda, South Sudan, the United Republic of Tanzania and Zambia; sporadic or travel-related cases have been reported in Angola, South Africa and Zimbabwe.
In settings where human-to-human transmission of mpox persists, the transmission is likely to be driven by a combination of sexual, household and community contacts. People move across country borders for reasons including labour migration, trade, family connections, and war and associated forced displacement. This cross-border mobility shapes epidemiological dynamics as well as the possibilities for effective preparedness and response. Within countries, the dynamics of transmission, access to care and containment strategies will be further shaped by the setting, including rural, hard-to-reach settings, informal settlements, camps for internally displaced people and refugees, and cross-border contexts. Although HBC presents specific challenges in these diverse settings, research suggests that community-based grassroots innovations are likely to emerge to protect others in times of adversity.4 Responders should work with these community-based innovations for an effective, community-led response.5
HBC for mpox in the context of ongoing transmission
Mpox is a viral disease, which can spread from animals to humans.6 Mpox mainly spreads between humans through close physical contact. Vaccination is recommended for people at high-risk of getting mpox, including healthcare workers.7 Most treatment for mpox is supportive to manage symptoms, such as aches, lesions and pain. Most people fully recover within a month without medical intervention. However, some infected people can get very sick and even die, and mpox can cause complications for children, pregnant women, people who are immunocompromised and people who suffer from chronic skin disease.8 The potential seriousness of the disease must be acknowledged when implementing HBC for mpox.
For mpox, HBC refers to care provided in the private home of a person with a probable or confirmed case of mpox. The caregiver may be a spouse, parent, other household member, friend or peer of the patient. People might isolate alone in their home or be able to do self-care, or both.
HBC involves varying levels of formal support. Many guidelines recognise the necessity to support HBC in epidemics for reasons such as insufficient capacity in formal healthcare settings; to reduce the risk of infection spread in health facilities; to cater for individuals’ potential preference for HBC, including in contexts where mistrust of health services (borne of historic exclusions and bad experiences or fear of stigma) is widespread;9 and people cannot afford healthcare. Formalising the use of HBC for mpox can help to better support mpox patients and carers by providing them with relevant information, hygiene kits, material, financial and psychosocial support, and the technical capacity to monitor clinical symptoms. The WHO recognises that,
‘Many people with mpox living in low-resource settings may have severely inadequate and insecure housing, often in contexts of overcrowding and poor sanitation, which increases the risk of exposure to infectious diseases and stress. Inadequate water supply and sanitation facilities affect personal hygiene. They also affect people’s ability to manage privacy and confidentiality. All of these create additional challenges during a mpox outbreak.’10
Preparedness and response strategies for mpox include plans and interventions for community protection at individual or household levels.11
Community protection refers to specific measures and strategies to safeguard a community and reduce risks and vulnerabilities regardless of the hazard. This can include policies, infrastructure development, emergency response planning, and community engagement initiatives. Community protection puts an emphasis on equity and accountability and the need to make a conscious effort to protect the health, well-being, and livelihoods of those at-risk or affected.12
At the individual or household level, public health advice typically includes assessing personal risk, preventing infection and providing advice for people with mpox to avoid the spread of infection, including when being cared for at home.
In the current mpox epidemic in Central and East Africa, transmission is known to happen through intra-family and intra-household contact. Furthermore, in eastern DRC, delayed care-seeking has been reported.13 A delay in seeking care is sometimes associated with difficulties in recognising mpox symptoms, together with limited screening capacity and long waiting periods to test samples and feedback results. This, in turn, leads to delayed isolation, contact tracing and clinical care.
Considering that health facilities may be out of reach for some people, and recognising limited resources and intra-household transmission, interventions to promote safety at home have largely focused on IPC and WASH measures. This focus highlights practical solutions to prevent the transmission of mpox during HBC and isolation at home.
Embedding HBC within existing health systems and community health services
HBC is a public health strategy of prevention, containment and care. It is necessarily connected to health systems and community health services, as well as less formal networks of care and solidarity.
Framing HBC as an arm of primary healthcare is essential. Incentives directed to vertical disease responses in emergencies can redirect priorities away from primary care strengthening.14 The tasks expected of healthcare workers in health emergencies sometimes impede the capacity of healthcare workers to deliver routine programmes. For example, research from Nigeria has shown that healthcare workers spent a lot of time filling out mpox contact forms, collecting samples and providing care at the expense of engaging with other health-related activities.14 Therefore, the tensions between mpox-specific services and approaches that integrate mpox responses into existing services should be acknowledged and accommodated in HBC guidelines.
Safe HBC ideally requires a functioning community-based referral system. In epidemic contexts where HBC is implemented to help isolate and manage mild mpox cases, carers and/or community health workers sometimes liaise with other community-based health programmes for mpox testing and contact tracing, for example. HBC as a model of care cannot function in a silo. HBC needs to be positioned within and/or alongside other forms of care that happen outside hospital settings. Although presented as ‘communal’, these other forms of care connect to national and local health systems, and they are not always aligned with grassroots ways of caring for others.
Figure 1 presents an illustrative pathway through which HBC connects to community-based strategies and referrals to health facilities.
HBC requires sufficient numbers of adequately trained and remunerated community health workers. The cadre of community health workers is wide-ranging and varies depending on contexts and health systems. Community health workers can include community members trained to assist locally with health prevention, communication and promotion, and community mobilisation. Community health workers sometimes assist with specific aspects of health delivery (e.g., to support underserved populations).15 Mpox responses highlight the potential of community health workers to support prevention and address misconceptions that hinder or delay people seeking healthcare or treatment and may disrupt surveillance activities.15 However, community health workers and volunteers are often overburdened, poorly remunerated and work within strained systems.
Figure 1. Community steps in detection, alert, investigation, home care, confirmation and referral
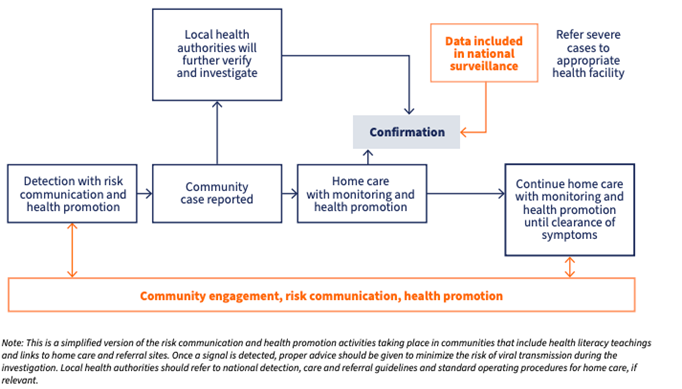
Source: Figure from Interim guidance on strengthening community detection and response during the mpox outbreak, 25 February 2025. Geneva: World Health Organization; 2025. https://doi.org/10.2471/B09313.
Learning from available IPC and WASH guidelines for mpox HBC and isolation in resource-limited settings
HBC for mpox has so far largely been informed by technical approaches focusing on IPC and WASH, as well as RCCE activities. In October 2024, the WHO and UNICEF published interim guidelines on IPC and WASH for HBC and isolation for mpox.16 The focus was on identifying ways to implement IPC in resource-limited settings. The guidance is presented as a bridge to limit community transmission when health facilities are overburdened or out of reach, and while clinical guidance is being reviewed. These guidelines are meant to be adapted nationally and locally.
Who is considered suitable for isolation and care at home?
According to the WHO and UNICEF guidelines,16 decisions to recommend isolation or HBC, or both, should be made by clinicians based on the severity, risk factors and care needed, as well as the person’s access to referral should complications from the mpox infection arise. People isolating at home should also have access to adequate food, water and hygiene. Access to social, economic and mental health support should also be considered. Pregnant women, people who are immunocompromised and children aged under five years should be cared for in a health facility as they are considered at higher risk for complications.16 Priority needs to be given to avoiding separating children from their parent(s) or carer(s) whenever possible.
IPC guidance at home, and alternatives when resources are scarce
Global mpox IPC guidance for HBC includes recommendations for isolating in a separate room. If a separate room is unavailable for the person with mpox, it is then recommended to clearly delineate a specific area within the shared space for the purpose of isolation.16
IPC measures also recommend that healthcare workers and/or community health workers who visit mpox patients at home should wear personal protective equipment (PPE) when or if entering into the isolation space or if a need arises (i.e., should a patient fall and need help).16 If PPE is not available, alternative options include avoiding entering a house and instead meeting outside whilst maintaining a one metre distance from the person with mpox. In the absence of PPE, other alternative barrier measures for the person with mpox include covering the lesions with a bandage or wearing loose-fitting clothes. If no medical mask is available, it is possible to use a fabric mask.
The IPC guidance also recommends that ideally only the person with mpox should handle and launder their bedding, clothing and other items. However, a designated caregiver, preferably vaccinated for mpox, may take the responsibility for these tasks if the person with mpox is unable to do so (e.g., a young child). When handling bedding or clothing, it is recommended to roll bedding rather than shake it out to prevent scattering infectious particles.17
WASH guidelines at home, and alternatives when resources are scarce
IPC guidelines for HBC emphasise the need to access clean WASH services.16 Access to running water and soap for cleaning hands is critical for HBC. Investment in WASH infrastructure should be prioritised whenever possible. Access to waste collection is not always available, and attention should be brought to minimising waste production. When sealed bags are not available to dispose of waste, it is recommended to dig a pit to empty waste downhill from any water source, away from animals and from areas where children play.18
Contextual adaptation of guidelines
Mpox transmission patterns and case fatality rates vary in different countries, partly reflecting differential access to care and support. There is also significant diversity in living arrangements and access to care between different settings within countries, such as urban and peri-urban settings, informal settlements, borderlands and remote rural areas. It is recognised that there is no ‘one size fits all’ response, including for the role of HBC and implementation of guidelines. Ideally, guidelines should be localised at subnational levels.
Implementation of guidelines in the context of multiple epidemics
Community health workers are routinely tasked to support people who are isolating at home and are often responsible for handling outbreaks of different diseases at the same time. This poses a range of challenges for HBC and for frontline responders; for example, PPE advice may differ depending on the particular disease (e.g., Ebola disease versus COVID-19).
Disease-specific responses can also hinder access to diagnosis. A syndromic approach to detection could enable several infections to be diagnosed at the same time. This approach could prevent measles being mistakenly diagnosed as mpox, for example, and enable a more integrated response, including the development of appropriate care plans and the implementation of the right IPC measures.
In Uganda, comorbidities compounding the severity of mpox include HIV. Uganda has therefore adapted protocols to integrate mpox and HIV for RCCE, testing and treatment; and case management experts are involved in managing treatment prioritisation. Among those presenting with both HIV/AIDS and mpox, males aged 30 to 49 years are the most affected, emphasising the need for integrated management strategies with the HBC approved by the strategic management team in the reporting period.19 Ensuring that patients receive care and are not turned away is essential no matter what the cause of their suffering is.
Broader social, economic and political issues to consider for HBC
HBC in the context of communal living spaces and infrastructures
Underlying assumptions about living arrangements may guide public health advice on isolating at home while waiting for a diagnosis or when recovering from an infection. In low-resource settings, homes may consist of a single room shared with several family members. This can make it difficult for a person with mpox to isolate from a caregiver and other household members. Also, there may be shared sanitation facilities or a complete lack of such facilities, which makes isolation and the implementation of IPC guidance challenging. Such contexts are rendered more complex by the lack of access to water and soap within the home. Women may also have to share a bed with their children.
In such a communal environment, there is emphasis on communal values, practices, and ideals. Children are not raised alone by their parents but with the influence of other elders in the compound, and in practice, this means that children are often in contact with others from different households.20
This means that HBC cannot always be contained to the household level, and each person’s right to confidentiality needs to be carefully balanced with HBC interventions.
Livelihood and service disruptions when isolating at home
Isolation can disrupt the livelihoods of people with mpox and their carers by restraining their movement, especially the poorer and more marginalised people who depend on daily wages or work in the informal sector. Without social security and safety nets, vulnerable households are left without an income to cover food and other basic needs, and cash transfers should be considered. Disruption of essential routine health services – such as maternal care, children’s health, routine immunisation, HIV treatment and chronic disease management – can threaten people’s health,21 while isolation of children disrupts learning and education. Integrating nutrition and health services, and providing children’s education at home during isolation, can help address these issues.22
Gendered practices of care and intersectional considerations for HBC
An understanding of how HBC may overburden women, including the most vulnerable women, is crucial for informing guidelines. HBC may add to already existing caring responsibilities and create new forms of gendered labour that occur in times of health emergencies;23 for example, as frontline workers involved in epidemic preparedness and response.24 Although mpox IPC guidelines state that infected adults should as much as possible disinfect the isolation area and change the linen themselves, for example, there are patriarchal settings where domestic work is considered the responsibility of women. These chores thus often are completed by women; for example, younger or unmarried women wash the laundry. These additional chores simultaneously increase women’s workloads and risk of exposure to infection.
Poverty also has a significant impact on out HBC. Basic commodities – such as several sets of linen and clothes, or clean water and soap – may not be available. Women who care for their children in addition to earning an income through informal work often do not have access to the financial safety nets or insurance or borrowing that would enable them to isolate or care. For example, women working in artisanal small mines in Kamituga, eastern DRC, face discrimination and typically occupy low-paid roles. This means that enforcing isolation at home for them or their children could lead to risky mitigation strategies.25
Stigma in the context of HBC for mpox
The sexual transmission of mpox caused by MPXV clade Ib has led to stigma and discrimination.26 In artisanal and small mining areas in the DRC, populations such as men who have sex with men, sex workers and migrants were identified early on in the mpox epidemic as being at higher risk and received particular attention in public health responses and prevention campaigns.25
Stigma while isolating at home was also a concern during the COVID-19 pandemic. Ethnographic research on HBC for COVID-19 in Gulu City, Uganda, revealed that stigma directed towards homes with people receiving COVID-19 HBC shaped the implementation of COVID-19 HBC strategy. Stigma forced many people with suspected and confirmed COVID-19 into hiding, thereby potentially endangering other community members. In order to protect the wider community from the dangers posed by those who were hiding, some local figures of public authority formed vigilante groups to oust cases.27
Confidentially of mpox status is important and follows lessons from other disease outbreaks. HBC visits for HIV patients were often perceived as problematic due to the risk of disclosure of HIV status. Recently, reports from the Ministry of Health in Uganda associates the rise of mpox with female sex workers and men who have sex with men – groups which have historically been stigmatised and criminalised. Consideration should therefore be given to ensuring confidentiality for people with mpox who need to isolate at home. Also, if a person’s mpox infection has become known in the community (e.g., through contact tracing), support should be provided to help the person reintegrate into the community after recovery.
Legacies of previous responses to epidemics
Previous experiences with epidemics such as Ebola disease and COVID-19 are likely to shape people’s understandings and responses to new epidemics, including their willingness to abide by regulations (e.g., isolating at home). Heavily securitised responses, for example, may be successful in enforcing compliance with interventions in the current outbreak, but they can risk breaking communities’ trust and buy-in. During COVID-19 lockdowns in Rwanda, most people respected and understood regulations, including stay-at-home orders. To enforce compliance, the government introduced fines and other punitive measures, which included forcing ‘offenders’ to stay overnight in a stadium for ‘education’ purposes and issuing lists of named ‘offenders’.28 Box 1 explores the legacies of COVID-19 in Uganda to further illustrate how heavy-handed measures, politicisation of the response and impunity for abuses of power can result in suspicion and fear, and ultimately rejection of interventions.
Box 1. Legacies of Uganda’s response to COVID-19 for mpox control
| The Ugandan government’s endeavour to contain and treat mpox, including the promotion of home-based care (HBC), is not dissimilar from the strategies deployed to contain and treat COVID-19.
In March 2020, a national task force for COVID-19 was established In Uganda. A command-and-control system was imposed with operations running through the Office of the Prime Minister.29 The task force was run by high-ranking military officials and civil servants. Together, they coordinated activities across complementary pillars.29 Input was also provided by international organisations, such as the World Health Organization; U.S. Centers for Disease Control and Prevention; UK Foreign, Commonwealth and Development Office; and UNICEF. This way of working was mirrored across the country. Indeed, COVID-19 task forces were established at district and sub-county levels, and eventually at a village level. Resident district commissioners (who are political appointees) chaired the district task forces, and district health officers were mandated to take the minutes. Police commanders and internal security officers also attended these meetings. The army has a role in the COVID-19 strategy. Initially, the role was limited to enforcing lockdowns by, for example, restricting movement within and between districts; overseeing the closure of schools, places of worship and markets; managing quarantine; preventing political rallies; and enforcing curfews.30 The army’s role expanded over the course of the epidemic, especially in Uganda’s borderlands.30 The deployment of soldiers to enforce COVID-19 vaccination among adults illustrates this: in parts of northwestern Uganda, for example, the army were reported to have beaten, caned and forcibly injected people with vaccines that they were often afraid to take. This approach fuelled anxieties that the COVID-19 vaccination campaign was part of a broader political project to kill or weaken groups that were already socially and politically marginalised.31 The overt politicisation of COVID-19 and the use of the army to enforce public health measures present challenges for those tasked with controlling mpox:
|
Source: Authors’ own.
Conflict and displacement
There are many reasons why people move across international borders, including displacement caused by natural disasters, war and conflict. Those fleeing violence are sometimes driven into overcrowded shelters and informal settlements, private rented accommodation, agricultural fields or schools, for example.32 Healthcare workers and community health workers are also affected by conflict and displacement, which can in turn affect their capacity, as well as that of the health system, to support HBC. Implementing protective measures in these circumstances is challenging and sometimes impossible. In dense settlements where HBC is not feasible (e.g., camps for internally displaced people and refugees), designated facilities can be designed or repurposed for isolation. However, public health responses will need to accommodate wider concerns including principles guiding protection in humanitarian spaces.33 Social, economic and political rights should inform HBC guidance.33 Furthermore, government authorities may not be perceived as legitimate in contexts of insecurity and/or marginalisation, and independent humanitarian actors on the ground, grassroots and refugee-led organisations, and trusted local leaders and representatives should be considered to facilitate HBC support, such as testing and contact tracing. During the COVID-19 pandemic, for example, refugee-led organisations successfully provided public health advice and healthcare delivery, and they played an important role in contact tracing while also monitoring human rights.34 It is important to re-evaluate the dynamics of legitimacy over time, as these are likely to change.33 Box 2 illustrates these points with reference to eastern DRC.
Box 2. Mpox home-based care and armed violence in eastern Democratic Republic of the Congo
| Armed violence in the eastern Democratic Republic of the Congo has caused the destruction of infrastructures, including hospitals and medical supplies. This destruction, combined with increased demand for care, can stretch already strained healthcare systems. Many health facilities in eastern Democratic Republic of the Congo are struggling to operate or have been destroyed, while ambulances have also been damaged or blocked from reaching affected areas. Health workers have had to flee, while others are working under life-threatening conditions, often with inadequate resources.
The Karanda Medical Center is located in the city of Kavumu, about 32 km from Bukavu. The medical centre regularly received patients, including suspected cases of mpox from surrounding rural areas. However, after M23 fighters took control of Kavumu Airport on 14 February 2025, medical staff and patients evacuated the mpox transit centre. The medical centre was subsequently looted, and ambulances were stolen. Although the medical centre has since been relocated to Businde, in the Miti-Murhesa health zone, patients have not returned. Some organisations have attempted to encourage patients to seek treatment by broadcasting radio announcements, but these efforts have been largely unsuccessful. Ongoing violence in the region – including gunfire – has led many patients to remain at home, particularly given the lack of essential supplies and food availability at the relocated medical centre. In South Kivu, home-based care is commonly practiced and often supported by doctors, herbalists and traditional healers. Many community health workers have fled due to increasing insecurity, and those who remain are often unpaid. Health centres in general – and mpox treatment centres in particular – have seen a sharp decline in operational capacity following the withdrawal of key partners (e.g., United States Agency for International Development, USAID). It remains unclear to what extent people with mpox may now be relying more heavily on informal healthcare systems and traditional medicine to manage mpox at home in this context. |
Source: Authors’ own.
Localising conceptions of care
Moral obligation to care for the sick. Situated logics of care, including the ‘oughtness’ to care for loved ones,35 sometimes translate into ignoring public health prevention and containment messaging in order to care for others in highly uncertain environments. For example, during the 2000–2001 Ebola disease outbreak in Gulu, northern Uganda, people prioritised making sure that their loved ones were being cared for, including by cleaning vomit or staying with their children in treatment centres, despite being aware of the risks for themselves.35 Elsewhere, it has been noted how moral obligations to care for those infected with Ebola during the 2013-2016 West African Ebola disease outbreak led communities to set aside national requirements to report possible cases. Instead, they created their own PPE and successfully treated people in secret, under the radar of official figures of public authority (e.g., paramount chiefs, humanitarian and national medical staff) attempting to respond to Ebola outbreaks.36
Formal and informal caregiving. Guidance and policies on HBC present connections between care at home and health systems, including through monitoring of symptoms by trained community health workers and healthcare workers, surveillance and contact tracing, and strategies to refer people at risk of developing complications to a health facility. However, caring for loved ones at home often unfolds in informal ways, without necessarily engaging with health services and public health guidelines. Mistrust in formal services can lead people to care for and protect loved ones outside official surveillance mechanisms.4 Fear of stigma associated with certain diseases can also reinforce informal HBC.
The tasks and hidden costs of caregiving at home. Caring for others at home entails a range of visible and hidden activities. Less visible tasks reported by people caring for people living with HIV in South Africa, for example, included spiritual support, showing love and compassion, household chores and making phone calls.37
Other networks of care and public authority. Networks of care connected to HBC may include less formal forms of authority that people trust and turn to, including to survive and cope in times of uncertainty or when relations between social groups (including marginalised social groups) and state infrastructures are weak. Parker and colleagues, for example, reported how mutuality between neighbours, linked to secret societies, enabled collective care for loved ones displaying signs of Ebola disease in rural parts of Sierra Leone. Care involved moving people from their homes to secret locations in nearby forests whilst ensuring they remained hydrated.4
Home treatments for mpox. It is not unusual for carers to create their own treatments for disease or to adapt treatments that have been used successfully in past outbreaks. In Sierra Leone, for example, a combination of lime, sugar and water was reported to have been successfully used to help rehydrate people infected with Ebola disease.4 With respect to mpox, Degoke and colleagues reported how bitter leaves, palm wine and black soap were used to alleviate symptoms.20
The impact of funding cuts on health services in the context of mpox and HBC
Recent reductions in international aid have significantly constrained the public health response to mpox, limiting access to essential services and placing additional strain on already fragile health systems. These cuts are affecting a broad range of health programmes across the African continent, including infectious disease surveillance and control, and they are likely to affect HBC. In the DRC, funding from the United States of America accounted for nearly 70% of all humanitarian aid in the past year. This support was crucial for activities such as the secure transport of suspected mpox samples from clinics to laboratories for testing. The withdrawal or reduction in funding, including to the Africa Centres for Disease Control and Prevention, is likely to jeopardises timely diagnosis of diseases and outbreak responses.38
At the continental level, innovative approaches are being pursued to boost domestic health spending and accelerate mpox response efforts through mechanisms like the Pandemic Fund. However, lessons from past epidemics highlight that prioritising global health security financing can disrupt essential health services.
Community health programmes have also been adversely affected by the funding cuts. Community health workers, who are central to outreach and response, now face increased pressures and limited resources to conduct their roles effectively, including providing support to people isolating at home. HBC for mpox may become more of a necessity as other services become overwhelmed.
References
- Kinganda-Lusamaki, E., Amuri-Aziza, A., Fernandez-Nuñez, N., Mbala-Kingebeni, P., Peeters, M., & Ahuka-Mundeke, S. (2025). Clade I mpox virus genomic diversity in the Democratic Republic of the Congo, 2018–2024: Predominance of zoonotic transmission. Cell, 188(1), 4–14. https://doi.org/10.1016/j.cell.2024.10.017
- Africa Centres for Disease Control and Prevention (Director). (2025, May 15). Special briefing on mpox and other health emergencies [Video recording]. https://www.youtube.com/watch?v=RsXJGFVLgns
- World Health Organization. (2025). Mpox: Multi-country external situation report no. 52 (Emergency Situational Updates). https://cdn.who.int/media/docs/default-source/documents/emergencies/multi-country-outbreak-of-mpox–external-situation-report–52.pdf?sfvrsn=bfb93ef0_3&download=true
- Parker, M., Matthew Hanson, T., Ahmed, V., Sao Babawo, L., & Allen, T. (2019). Ebola, community engagement, and saving loved ones. The Lancet, 393(10191). https://doi.org/10.1016/S0140-6736(19)31364-9
- Richards, P. (2016). Ebola: How a people’s science helped end an epidemic. Zed Books.
- World Health Organization. (n.d.). Mpox. Retrieved 23 May 2025, from https://www.who.int/health-topics/mpox
- World Health Organization. (2024, August 26). Mpox: Key facts. https://www.who.int/news-room/fact-sheets/detail/mpox
- United Nations Children’s Fund (UNICEF). (2024). Guidance for RCCE practitioners on mpox. https://www.rcce-collective.net/wp-content/uploads/2024/12/Guidance_for_RCCE_practitioners_on_Mpox.pdf
- MacGregor, H., & Hrynick, T. (2020). Covid-19 considerations for home and community-based care. Social Science in Humanitarian Action Platform. https://www.socialscienceinaction.org/resources/covid-19-considerations-home-community-based-care/
- World Health Organization. (2024). Public health advice for people recovering from or caring for someone with mpox at home in low-resource settings. https://www.who.int/publications/m/item/public-health-advice-for-people-recovering-from-or-caring-for-someone-with-mpox-at-home-in-low-resource-settings
- World Health Organization. (2025). Interim guidance on social and behavioural research for the mpox public health response. https://iris.who.int/bitstream/handle/10665/380881/B09339-eng.pdf?sequence=1
- World Health Organization. (2024). Defining community protection: A core concept for strengthening the global architecture for health emergency preparedness, response and resilience. https://iris.who.int/handle/10665/379055
- Adigun, O. A., Okesanya, O. J., Ahmed, M. M., Ukoaka, B. M., Lucero-Prisno III, D. E., Onyeaghala, E. O., Oluwasusi, E. A., Ogunwale, O. E., & Faniyi, A. A. (2024). Syndemic challenges: Addressing the resurgence of mpox amidst concurrent outbreaks in the DRC. Transboundarey and Emerging Diseases, 1962224. https://doi.org/10.1155/tbed/1962224
- Schmidt-Sane, M., Adegoke, O., Abbas, S., Lawanson, A. O., Kunnuji, M., Jegede, A., & MacGregor, H. (2024). Infrastructures of epidemic response: Mpox and everyday repair work in southwestern Nigeria. Social Science & Medicine, 358. https://doi.org/10.1016/j.socscimed.2024.117246
- Schneider, H., Dickson, O., & Lehmann, U. (2016). The global pendulum swing towards community health workers in low- and middle-income countries: A scoping review of trends, geographical distribution and programmatic orientations, 2005 to 2014. Human Resources for Health, 14(65). https://doi.org/10.1186/s12960-016-0163-2
- World Health Organization & United Nations Children’s Fund (UNICEF). (2024). Infection prevention and control and water, sanitation and hygiene measures for home care and isolation for mpox in resource-limited settings: Interim operational guide. World Health Organization. https://iris.who.int/handle/10665/379477
- GWC Hygiene Promotion Working Group, CAST, UNICEF, IFRC, Save the Children, & Tufts University. (2024). Guidance for WASH practitioners on mpox. Wash cluster. https://www.washcluster.net/sites/gwc.com/files/inline-files/Mpox%20brief_v4.pdf
- United Nations Children’s Fund (UNICEF). (2025). Burundi Mpox Level 3 Emergency (Humanitarian Situation Report 5). UNICEF. https://www.unicef.org/media/166936/file/Burundi-Humanitarian-SitRep-Mpox-31-December-2024.pdf
- UNICEF. (n.d.). Humanitarian Situation Report No. 5: Uganda Mpox Level 3 Emergency. https://www.unicef.org/media/169026/file/UNICEF%20Uganda%20Humanitarian%20Situation%20Report%20No.%205%20%20(Mpox%20)%201%20-%20Jan%20-%2028%20February%202025.pdf.pdf
- Adegoke, O., Schmidt-Sane, M., Kunnuji, M., Abbas, S., Lawanson, A., Jegede, A., & MacGregor, H. (2025). Diagnosis, treatment, and management of Mpox in urban informal settlements in Southwestern Nigeria: An ethnographic approach. BMC Public Health, 25(115). https://doi.org/10.1186/s12889-024-21267-1
- World Health Organization. (2024, December 3). Maintaining essential health services amid mpox outbreak response. https://www.afro.who.int/news/maintaining-essential-health-services-amid-mpox-outbreak-response
- World Health Organization. (2024). Community protection for the mpox response: A comprehensive set of actions [Community protection technical brief series]. https://doi.org/10.2471/B09182
- Schmidt-Sane, M., Nielsen, J., Chikombero, M., Lubowa, D., Lwanga, M., Gamusi, J., Kabanda, R., & Kaawa-Mafigiri. (2022). Gendered care at the margins: Ebola, gender, and caregiving practices in Uganda’s border districts. Global Public Health, 17(6), 899–911. https://doi.org/10.1080/17441692.2021.1879895
- Kingori, P., Kombe, F., & Fehr, A. (2022). Making global health ‘work’: Frontline workers’ labour in research and interventions. Global Public Health, 17(12). https://doi.org/10.1080/17441692.2022.2139852
- Bashwira, M.-R., Mihigo, I. M., & Duclos, D. (2024). Key considerations: Mpox, mining, and vulnerabilities of women and children in eastern DRC. Social Science in Humanitarian Action Platform. https://www.socialscienceinaction.org/resources/key-considerations-mpox-mining-and-vulnerabilities-of-women-and-children-in-eastern-drc/
- Duclos, D., & MacGregor, H. (2024). Meeting report: Mpox and discrimination in African settings. Social Science in Humanitarian Action Platform. https://www.socialscienceinaction.org/resources/meeting-report-mpox-and-discrimination-in-african-settings/
- Okello, R., Duclos, D., & Parker, M. (n.d.). Rethinking home-based care during epidemics: Reflections from Gulu, northern Uganda during an outbreak of COVID-19.
- Luther Munu, M., & Vlaminck, Z. (2021). Beyond the curve: Equity in Rwanda’s COVID-19 response. INCLUDE. https://includeplatform.net/wp-content/uploads/2021/05/COVID-report-Rwanda-.pdf
- Parker, M., MacGregor, H., & Akello, G. (2020). Covid-19, public authority and enforcement. Medical Anthropology: Cross-Cultural Studies in Health and Illness, 39(8), 666–670. https://doi.org/10.1080/01459740.2020.1822833
- Parker, M., Baluku, M., Ozunga, B. E., Okello, B., Kermundu, P., Akello, G., MacGregor, H., Leach, M., & Allen, T. (2022). Epidemics and the military: Responding to COVID-19 in Uganda. Social Science & Medicine, 314, 115482. https://doi.org/10.1016/j.socscimed.2022.115482
- Parker, M., Okello, B., Kermundu, P., Ozunga, B. O., Baluku, M., Akello, G., MacGregor, H., Leach, M., & Allen, T. (n.d.). Did COVID-19 vaccine enforcement work? Evidence from north-western and northern Uganda. [Manuscript Submitted for Publication].
- United Nations High Commissioner for Refugees (UNHCR). (2024, August 27). Concerned over impact of mpox on refugees and displaced in Africa, UNHCR calls for inclusion and international solidarity. https://www.unhcr.org/uk/news/briefing-notes/concerned-over-impact-mpox-refugees-and-displaced-africa-unhcr-calls-inclusion
- Mylan, S. (2025). Protection and containment: Surviving COVID-19 in Palabek Refugee Settlement, Northern Uganda. Global Policy, 16(1). https://doi.org/10.1111/1758-5899.13496
- Betts, A., Easton-Calabria, E., & Pincock, K. (2021). Localising public health: Refugee-led organisations as first and last responders in COVID-19. World Development, 139. https://doi.org/10.1016/j.worlddev.2020.105311
- Park, S.-J., & Akello, G. (2017). The oughtness of care: Fear, stress, and caregiving during the 2000–2001 Ebola outbreak in Gulu. Social Science & Medicine, 194, 60–66. https://doi.org/10.1016/j.socscimed.2017.10.010
- Parker, M., Hanson, T. M., Vandi, A., Babawo, L. S., & Allen, T. (2019). Ebola and public authority: Saving loved ones in Sierra Leone. Medical Anthropology, 38(4), 1–15. https://doi.org/10.1080/01459740.2019.1609472
- Akintola, O. (2006). Gendered home-based care in South Africa: More trouble for the troubled. African Journal of AIDS Research, 5(3), 237–247. https://doi.org/10.2989/16085900609490385
- Stone, W., & Huang, P. (2025, February 25). Upheaval and firings at CDC raise fears about disease outbreak response. NPR. https://www.npr.org/sections/shots-health-news/2025/02/25/nx-s1-5307117/cdc-firings-infectious-disease-response
Authors: Diane Duclos (London School of Hygiene and Tropical Medicine), Bob Okello (Independent Consultant, Gulu, Uganda), Godefroid Muzalia (Le Groupe d’Etudes Sur Les Conflits el al Sécurité Humaine, DRC) and Melissa Parker (London School of Hygiene and Tropical Medicine).
Acknowledgements: The brief was reviewed internally reviewed by Megan Schmidt-Sane (Institute of Development Studies) and Hayley MacGregor (Institute of Development Studies), and externally reviewed by Nadine Beckman (London School of Hygiene and Tropical Medicine, and UK Public Health Rapid Support Team), Anthony Twyman (Senior Infection Prevention and Control Specialist for UK Public Health Rapid Support Team, UK Health Security Agency) and Gillian McKay (Elrha). Editorial support was provided by Harriet MacLehose. This brief is the responsibility of SSHAP.
Suggested citation: Duclos, D., Okello, B., Muzalia, G. and Parker, M. (2025). Key considerations: Home-based care for mpox in Central and East Africa. Social Science in Humanitarian Action Platform (SSHAP). www.doi.org/10.19088/SSHAP.2025.026
Published by the Institute of Development Studies: May 2025.
Copyright: © Institute of Development Studies 2025. This is an Open Access paper distributed under the terms of the Creative Commons Attribution 4.0 International licence (CC BY 4.0). Except where otherwise stated, this permits unrestricted use, distribution, and reproduction in any medium, provided the original authors and source are credited and any modifications or adaptations are indicated.
Contact: If you have a direct request concerning the brief, tools, additional technical expertise or remote analysis, or should you like to be considered for the network of advisers, please contact the Social Science in Humanitarian Action Platform by emailing Annie Lowden ([email protected]) or Juliet Bedford ([email protected]).
About SSHAP: The Social Science in Humanitarian Action (SSHAP) is a partnership between the Institute of Development Studies, Anthrologica , CRCF Senegal, Gulu University, Le Groupe d’Etudes sur les Conflits et la Sécurité Humaine (GEC-SH), the London School of Hygiene and Tropical Medicine, the Sierra Leone Urban Research Centre, University of Ibadan, and the University of Juba. This work was supported by the UK Foreign, Commonwealth & Development Office (FCDO) and Wellcome 225449/Z/22/Z. The views expressed are those of the authors and do not necessarily reflect those of the funders, or the views or policies of the project partners.
Keep in touch
Email: [email protected]
Website: www.socialscienceinaction.org
Newsletter: SSHAP newsletter

